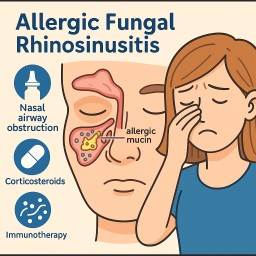
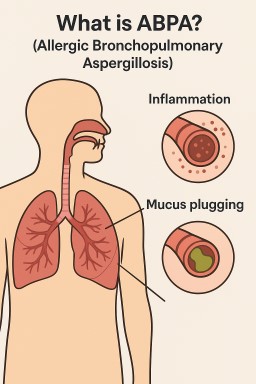
(Also called Allergic Fungal…
by GAtherton
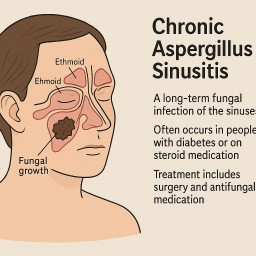
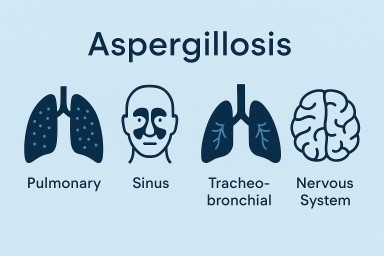
(Chronic invasive and…
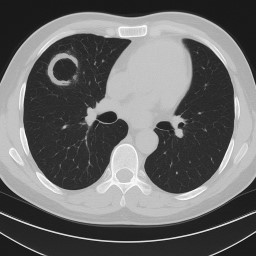
Aspergilloma (Fungal Ball in…
Print out or share…
Print this off or share…
Patient handout for A&E…
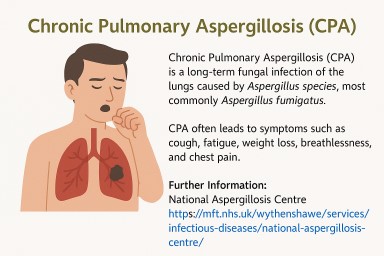
Some people with chronic…
If you have aspergillosis,…
👃 What Is AFRS? Allergic…