It’s quite possible for…
by GAtherton
Many people living with…
Question: “I have…
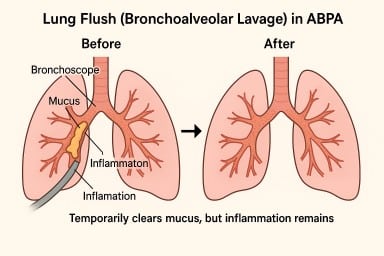
A lung flush (also called a…
Many people with asthma, ABPA…
Many patients with ABPA,…
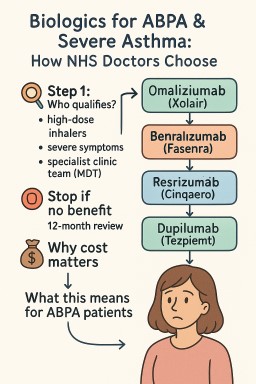
Biologics are modern…
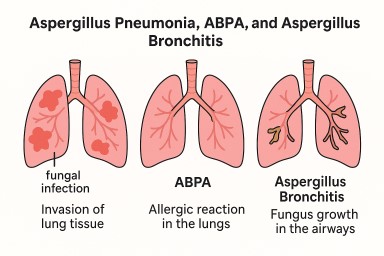
What is it? Aspergillus…