Conditions
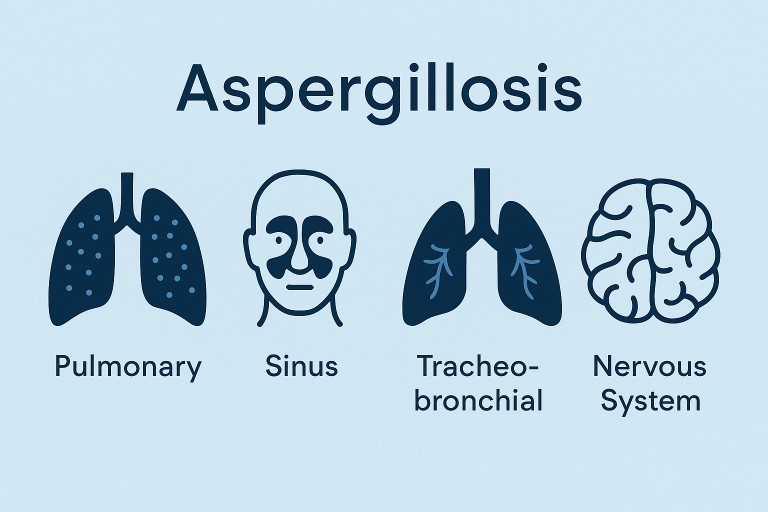
👁️ Other forms of Aspergillosis: Aspergillus Endophthalmitis, A Rare Eye Infection
🧐 What Is It? Aspergillus…
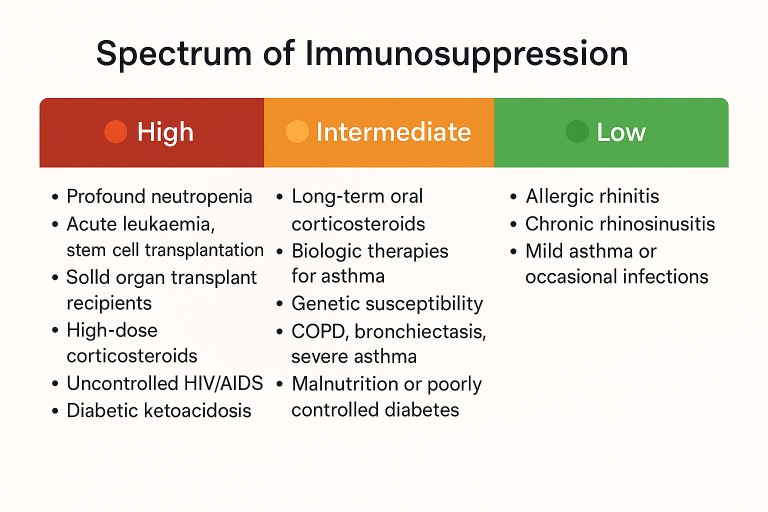
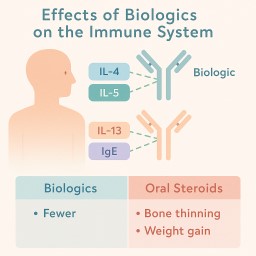
🛡️ Understanding Your Risk: Aspergillosis, Steroids, and the Immune System
If you’ve been diagnosed with…
Other forms of Aspergillosis: 🔬 Acute Invasive Aspergillus Sinusitis (AIAFS)
⚠️ A rare and severe fungal…