Research Summaries
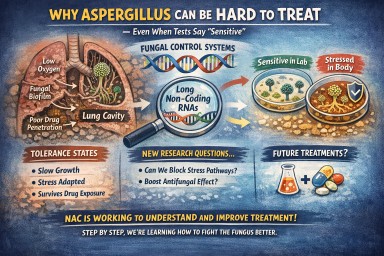
Why Can Aspergillus Infection Be Hard to Clear — Even When Tests Say It’s “Sensitive”?
Many patients ask: “If my…
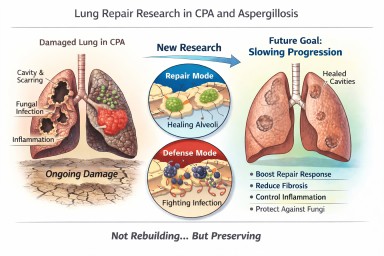
Looking further into the future - could we control lung damage, preserve healthy lung tissue better?
Can Lungs Repair Themselves?…
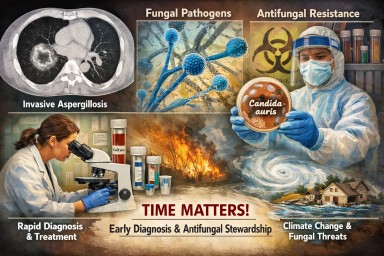
Systemic fungal infections: why speed, diagnosis and stewardship matter
Systemic fungal infections —…

Can blood tests help predict if chronic pulmonary aspergillosis will come back?
This study from the National…

Connecting patients, carers, clinicians and scientists to improve life with aspergillosis
World Aspergillosis Day (WAD)…