Specialist evidence briefing:…
by GAtherton
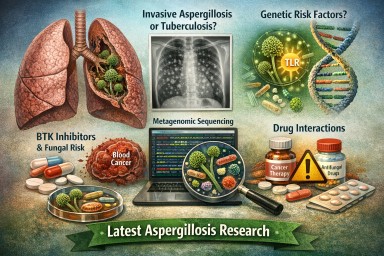
Key message: Commercial…
Key message: Chronic…
This week’s PubMed search for…
Search term: aspergillosis…
Highlights this week…
This week’s papers point in…
Last reviewed: April 2026…