🫁 ABPA Treatment: Why Are Steroids First, Even if They Can Increase Fungal Growth?

If you've been diagnosed with Allergic Bronchopulmonary Aspergillosis (ABPA), you may have heard that treatment often starts with oral steroids like prednisolone. But ABPA is triggered by a reaction to the Aspergillus fungus — so why use a treatment that might actually let that fungus grow more?
It’s a great question. This guide explains why steroids are still often the first step, what other treatments are available, and when they might be used.
🌿 What Is ABPA?
ABPA is not an infection — it’s an allergic immune reaction in the lungs to the fungus Aspergillus fumigatus. This overreaction causes:
-
Lung inflammation
-
Mucus plugging
-
Breathlessness and wheezing
-
Possible long-term lung damage (e.g., bronchiectasis)
People with asthma or cystic fibrosis are more likely to develop ABPA.
💊 Why Are Steroids Usually the First Treatment?
🔥 The key problem in ABPA is inflammation, not the fungus itself.
Steroids like prednisolone are often used first because they:
-
Act quickly to calm the allergic immune reaction
-
Reduce inflammation and mucus
-
Help relieve symptoms fast (wheezing, tight chest, breathlessness)
-
Prevent long-term damage if started early
Even though steroids may allow some fungal growth, their fast action against inflammation is often more important — especially in flare-ups.
🍄 What About Antifungal Treatments?
Antifungals like itraconazole or posaconazole reduce the amount of Aspergillus in the lungs. This helps to:
-
Reduce allergic triggers
-
Prevent future flare-ups
-
Lower the need for steroids
However, antifungals:
-
Take weeks to work
-
Don’t control inflammation well on their own during a flare
-
Can have side effects and interact with other medications
➡️ That’s why they are often used after steroids, or alongside them — especially in people who flare up often or need steroids long term.
🧬 What About Biologics?
Biologic therapies like:
-
Omalizumab (anti-IgE)
-
Dupilumab (blocks IL-4 and IL-13)
-
Mepolizumab (anti-IL-5)
…are used to help regulate the immune system in patients who:
-
Can’t tolerate steroids
-
Have frequent relapses
-
Need ongoing treatment despite antifungals
Biologics can help:
-
Reduce steroid use
-
Lower flare frequency
-
Improve asthma control
But they’re not yet approved as first-line treatments and are generally reserved for more complex or persistent cases.
✅ What Happens If My Symptoms Are Mild?
Good question. In mild ABPA (e.g. stable breathing, low IgE, no major lung damage), specialists may:
-
Monitor closely before starting any treatment
-
Try antifungals alone, especially if steroid use is risky
However, regular follow-up is essential to make sure inflammation doesn’t silently worsen.
🔄 Typical ABPA Treatment Steps
| Stage | Treatment |
|---|---|
| First flare or moderate symptoms | Steroids (short course) ± antifungals |
| Steroid side effects or long-term use | Add antifungals |
| Recurrent or steroid-dependent ABPA | Add or switch to biologics |
| Mild symptoms and stable lungs | Possibly antifungals first (specialist decision) |
🧘 Staying Well with ABPA
-
Follow your treatment plan closely
-
Keep lungs clear with mucus clearance techniques
-
Avoid damp, mouldy environments
-
Keep up with regular check-ups and lung tests
-
Let your team know if symptoms return
🗨️ In Summary
Steroids are still first-line because they work fast to stop inflammation.
Antifungals and biologics are important longer-term options that help reduce fungal triggers and flare-ups — and may reduce or even replace steroids over time.
Every ABPA patient is different, and your care should be tailored to you.
🫁 Understanding ABPA, Bronchiectasis & Lung Cavities
A Patient’s Guide to What Happens in the Lungs – and What You Can Do About It
🌿 What is ABPA?
Allergic Bronchopulmonary Aspergillosis (ABPA) is a condition where the lungs react strongly to a common fungus called Aspergillus. This overreaction causes inflammation in the airways, making it harder to clear mucus and increasing the risk of flare-ups.
Many people with asthma or cystic fibrosis are more likely to develop ABPA, but it can affect others too.
🌀 What Happens to the Lungs?
Over time, repeated inflammation and mucus build-up can affect the structure of the airways. Here’s what can happen:
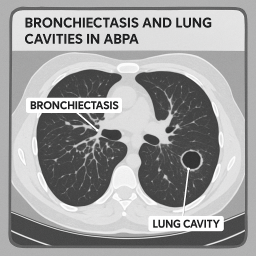
1. Bronchiectasis
-
The airways (bronchi) become widened and thickened.
-
This makes it harder to clear mucus, which can lead to more infections.
-
In ABPA, this usually affects the central parts of the lungs.
🔸 Bronchiectasis is not the same as a lung cavity. It’s a change in the shape of the airways, not a hole in the lung.
2. Lung Cavities (Less Common)
-
These are air-filled spaces that form when a small area of lung tissue is damaged or infected.
-
Cavities are less common in ABPA but can happen after repeated inflammation or infection.
-
They may look worrying on a scan, but often they are just monitored and don’t cause major issues unless they become infected.
🩺 What About Lung Function?
ABPA and bronchiectasis can affect lung function, especially if not caught early.
-
Spirometry tests may show lower results if the airways are blocked or inflamed.
-
Some people improve after treatment; others may see a gradual decline.
-
Most patients still breathe well at rest, and many stay active with proper care.
🌬️ Will Cavities Leak Air?
This is a common worry. The answer is: usually not.
-
Most cavities in ABPA are not at risk of bursting or leaking.
-
Sudden breathlessness or chest pain should always be checked, but leaks (pneumothorax) are rare in ABPA.
📉 Does Everyone Get Cavities?
Not at all.
-
Around 50–90% of ABPA patients get some bronchiectasis.
-
Only a minority go on to develop true cavities.
-
Early treatment and regular check-ups help reduce the risk of further lung changes.
🧪 What About Oxygen Levels?
Many people with ABPA — even with bronchiectasis — still have normal oxygen levels (SpO₂):
-
Most rest between 95–98%
-
During a flare or infection, it might dip a little
-
If oxygen drops below 92%, your team may check more closely
🧘 What Can I Do to Stay Well?
-
🩺 Stick to your treatment plan – antifungals, inhalers, or steroids if prescribed
-
💨 Clear mucus regularly – ask about airway clearance techniques
-
🧼 Avoid damp, mouldy environments
-
🍎 Stay active and eat well
-
📆 Attend check-ups and lung function tests
-
🚭 Avoid smoking or vaping (these can worsen damage)
💬 A Final Word
Having ABPA and some lung changes doesn’t mean life has to stop. Many people continue to live active, fulfilling lives. Even with bronchiectasis or small cavities, the focus is on prevention, staying stable, and getting support when needed.
📘 Managing IgE Levels in ABPA: What Happens After Treatment?
If you have ABPA (Allergic Bronchopulmonary Aspergillosis), you’ve likely been told your IgE levels are high. Many patients ask:
“Once my IgE goes down with treatment, how do I keep it down without staying on steroids or antifungals forever?”
This guide explains why IgE is important, how it’s treated, and what long-term steps you can take to stay well.
🧪 What is IgE and Why Is It High in ABPA?
IgE (Immunoglobulin E) is an antibody your immune system makes in response to allergens. In ABPA, your immune system overreacts to Aspergillus, a common fungus, causing inflammation in the lungs. This leads to:
-
High total IgE levels (often over 1,000–10,000 IU/mL)
-
Symptoms like coughing, wheezing, and mucus plugs
-
Lung changes on scans, if untreated
🎯 Treatment Goals
Treatment aims to:
-
Lower inflammation
-
Reduce the fungal burden
-
Bring IgE levels down (a marker that your inflammation is settling)
-
Prevent long-term lung damage
You might be treated with:
-
Oral steroids (e.g. prednisolone)
-
Antifungal tablets (e.g. itraconazole or voriconazole)
These medications help bring IgE levels down, sometimes dramatically. But they can’t usually be taken forever — long-term use may cause side effects.
🔄 After IgE Drops – What Next?
Even after successful treatment, ABPA can flare up again. So the key questions become:
How do we keep IgE low?
How do we prevent future flare-ups?
🧭 Long-Term Management Options
1. Close Monitoring
-
IgE is checked every 2–6 months
-
Doctors look for a doubling in IgE — this can mean a flare is starting
-
Regular chest scans and lung function tests are also used to spot changes early
2. Tapering Medication
-
Steroids are slowly reduced, not stopped suddenly
-
Your doctor will watch for any return of symptoms or rise in IgE
3. Biologic Treatments
Some newer medications can help long-term, especially if you:
-
Have frequent flare-ups
-
Can’t reduce steroids safely
-
Have asthma or eosinophilic inflammation
These include:
-
Omalizumab (anti-IgE antibody)
-
Mepolizumab / Benralizumab (target eosinophils)
-
Dupilumab (blocks part of the allergy pathway)
Biologics are usually injections given every 2–4 weeks, and can help reduce relapses and steroid need.
🏡 Lifestyle & Environmental Tips
Reducing your exposure to Aspergillus can help keep IgE from rising again.
🔹 Avoid:
-
Damp or moldy areas
-
Compost, rotting leaves, hay, or soil dust
-
Rooms with poor ventilation
🔹 Use:
-
Ventilate your home well (eg open windows/extractor fans)
-
A HEPA-filter air purifier at home
-
An FFP2/FFP3 mask when doing dusty activities (gardening, cleaning mold)
🥗 Eat for Immune Support:
-
Anti-inflammatory foods (vegetables, oily fish, berries)
-
Reduce sugar (high sugar may promote inflammation)
-
Stay well hydrated
-
Ask your doctor about vitamin D — it may help regulate immunity
📅 Follow-up Schedule (General examples, yours may differ)
| Time Since Treatment | What to Expect |
|---|---|
| 1–3 months | Blood tests (IgE, eosinophils), lung check |
| 3–6 months | Check for symptoms, possibly repeat IgE |
| 6–12 months | CT scan or lung function, if needed |
| After 1 year | Stable patients may have annual reviews |
Let your team know if any symptoms return — even if your last IgE result was stable.
🧠 Final Thoughts
-
You may always have “elevated” IgE compared to someone without ABPA — that’s okay. The goal is stability, not “zero IgE”.
-
Many patients live well with ABPA for years by learning to manage flare-ups early and avoiding fungal exposure.
-
Ask your clinic about your personal IgE pattern — some people flare with small changes; others don’t.
-
Support groups and educational resources (like aspergillosis.org) can help you stay informed and confident.
📩 Have questions for your team?
Bring these up at your next appointment:
-
Can I reduce my medication safely?
-
Could I benefit from a biologic?
-
How often should I check my IgE?
-
How can I reduce exposure at home?
🏠 NICE Guidance on Damp and Mould (NG149) — Simple Summary
1. Health Risks
-
Damp and mould produce spores and irritants that can trigger or worsen respiratory and heart conditions, including asthma, bronchitis, and fungal infections, like aspergillosis Link
-
They can also affect skin, eyes, and mental wellbeing, especially in vulnerable people such as those with asthma, COPD, babies, pregnant women, and older adults .
2. When Health Issues Worsen
If you experience repeated cough, wheeze, or other breathing issues — and your home has damp or mould — health professionals are advised to:
-
Ask about your home conditions
-
Help you arrange a housing assessment by the council Link
3. Landlord and Council Responsibilities
Landlords and councils should:
-
Act quickly and sensitively when damp or mould is reported — medical proof is not required Link
-
Identify and fix the root cause (e.g., faulty guttering leading to mould) — not just clean it off Link.
-
Keep clear records, follow up after repairs, and inspect properties periodically to prevent recurrence Link
4. Tenant Health Priority
Homes with serious damp and mould are classed as Category 1 hazards under UK housing law, meaning they pose an immediate health risk. Councils must act — they can enforce repairs, impose notices, or carry out work themselves Link.
5. How You Can Use This with Your Council
-
Point to NICE NG149 guidance to emphasise that damp and mould are a legal and health priority.
-
Remind them that action must be urgent, especially for people with lung conditions.
-
Ask them to identify and fix the cause, not just scrub the mould — like ensuring guttering is repaired and mould-prone areas are treated and dried.
-
Ask for a follow-up inspection to confirm the problem is resolved.
📩 Suggested Wording to Share with Your Council
“According to NICE guidance (NG149), damp and mould in homes are considered serious health hazards — especially for people with lung conditions like aspergillosis. Councils and landlords must act quickly to fix the root cause, not just remove visible mould. These guidelines recognise that even without medical proof, urgent action is required to protect tenants’ health.”
🏥 Can a GP Refer You Directly to the National Aspergillosis Centre (UK)?
❌ Unfortunately, no — not directly.
The NAC is a tertiary referral centre, meaning that:
-
Referrals must come from a hospital consultant (usually a respiratory or infectious diseases specialist)
-
The NAC cannot accept direct referrals from GPs or from patients themselves
This is due to NHS policy and service structure — not because they don’t want to help.
✅ What Your GP Can Do:
Even though they can’t refer you directly, your GP can advocate on your behalf and help move things forward by:
-
Writing to your current hospital consultant to request:
-
A second opinion from NAC
-
Transfer of care or joint management with NAC
-
Review of your images, sputum results, and previous history
-
-
If your current hospital won’t cooperate, your GP can:
-
Refer you to a different respiratory consultant (at another hospital if needed)
-
Ask that this new consultant considers NAC referral
-
-
If your case involves rare, persistent, or poorly controlled lung disease with suspected Aspergillus involvement, the NAC is usually happy to review — but only after that consultant request is made.
📂 What to Send (via the consultant)
Your hospital team (at your GP’s request) should ideally send:
-
Latest CT scans and chest X-rays
-
Sputum culture results
-
Total and specific IgE / Aspergillus IgG
-
A clear clinical history summary
-
Any previous diagnosis letters or clinic notes
🗣️ If You’re Still Not Getting Help
If your current consultants won’t help and your GP is willing, you might also:
-
Ask your GP to refer you to a private respiratory specialist (for one appointment only) who may agree to refer you to NAC from there.
-
Or contact your local Patient Advice and Liaison Service (PALS) to escalate the block in access.
💬 Suggested Wording for Your GP:
“I’ve had long-standing respiratory symptoms with suspected Aspergillus involvement and limited progress under my current hospital team. I understand referral to the National Aspergillosis Centre requires a hospital consultant, but would you be willing to request that my current team (or an alternative respiratory consultant) considers this referral on my behalf?”
💡 Summary:
-
❌ GPs cannot refer you directly to NAC
-
✅ Your GP can request your hospital consultant do it — and advocate for you
-
🛑 If you're being blocked, ask to be referred to another consultant who may be more open to referring to NAC
🕵️♀️ Protecting Your Privacy as a Member of National Aspergillosis Centre Support (UK)
A guide for staying anonymous outside the group while still taking part inside
The National Aspergillosis Centre Support (UK) Facebook group is a private but visible group. That means:
-
Only members can see your posts, comments, and activity inside the group
-
But anyone on Facebook can find the group name, description, and see how many members it has
-
And people who visit the group page (such as your friends or the public) may see your name and profile photo in the member list
This is a safe, supportive space — but we understand that some members prefer to keep their involvement private from friends, family, employers, or the wider Facebook community.
Here’s how you can protect your privacy and remain as anonymous as you wish outside the group.
🔐 What Is Visible to Non-Members?
Non-members (including your Facebook friends) cannot see:
-
Any posts, comments, photos, or questions you share in the group
-
Who you’re interacting with in the group
-
What you react to or how often you post
But they can see:
-
That you are a member of the group (if they visit the group page)
-
Your name and profile picture in the group member list
-
That the group is titled “National Aspergillosis Centre Support (UK)” — which some people prefer to keep private
✅ How to Protect Your Identity Outside the Group
1. 🧑💻 Use a Privacy-Conscious Name
You can use a shortened or modified version of your real name, such as:
-
First name + middle name
-
A shortened surname (e.g. Jane S. or Jo Samuel)
-
A pseudonym that still sounds plausible
⚠️ Avoid completely fake names (e.g. “Invisible Fungus”) — Facebook may flag them.
2. 🖼️ Choose a Neutral Profile Picture
Instead of a facial photo, consider using:
-
A photo of nature
-
A quote or piece of artwork
-
A blurred or abstract image
This helps maintain your privacy if someone visits the group member list.
3. 🔧 Adjust Your Facebook Privacy Settings
Go to Settings & Privacy > Settings > Privacy and update the following:
| Setting | Recommended |
|---|---|
| Who can see your friends list? | Only Me |
| Who can look you up using email/phone? | Only Me |
| Do you want search engines to link to your profile? | No |
| Who can see what others post on your timeline? | Only Me |
| Who can see posts you’re tagged in? | Only Me |
4. 👤 Hide the Group from Your Profile
Even though this is a private group, Facebook may show it on your profile under "Groups."
To remove it:
-
Go to your profile
-
Scroll to the Groups section
-
Click the three dots (…) next to “National Aspergillosis Centre Support (UK)”
-
Select “Hide from profile”
5. 🙈 Use Anonymous Posting for Sensitive Questions (If Enabled)
We are exploring whether anonymous posting can be enabled in the group. When switched on:
-
Other members see your post as “Anonymous Member”
-
Admins and moderators can still see who posted for safety reasons
Let an admin know if this feature would be helpful for you.
6. 📱 Avoid Linking Your Activity to Outside Apps or Pages
-
Don’t share group posts on your timeline (they won’t be visible, but it may confuse others)
-
Avoid linking group activity to external apps (like Instagram or other health platforms)
-
Use caution when interacting with group members on your public profile
🧾 Summary: Stay Anonymous Outside the Group
| Tip | Why It Helps |
|---|---|
| Use a modified or shortened name | Reduces traceability outside the group |
| Use a neutral profile image | Makes you harder to identify in the group list |
| Change privacy settings | Stops Facebook from exposing your activity or connections |
| Hide group from your profile | Prevents others from seeing your group involvement |
| Use anonymous posting (if available) | Keeps your name hidden in sensitive discussions |
💬 Final Note from the Admin Team
We understand that aspergillosis is a sensitive condition, and you have every right to protect your identity while still seeking support. This group exists to help — safely, kindly, and confidentially. If you’re ever unsure about how your name or photo appears, or you need support to adjust your settings, please message one of the admin team privately. We’ll help however we can.
Understanding the Different Types of Chronic Pulmonary Aspergillosis (CPA)
CPA is a long-term lung condition caused by a common fungus called Aspergillus. It usually affects people who already have lung damage — from infections like tuberculosis (TB), conditions like COPD or asthma, or diseases such as sarcoidosis.
There are five main types of CPA. Knowing which one you have can help guide your treatment and follow-up.
🟠 1. Chronic Cavitary Pulmonary Aspergillosis (CCPA)
Most common form
-
Caused by Aspergillus growing in one or more cavities in the lungs
-
Cavities may slowly get larger or thicker
-
Often develops in people with previous lung disease
Symptoms:
-
Long-term cough
-
Fatigue and weight loss
-
Breathlessness
-
Sometimes mild or moderate coughing up blood
Treatment: Long-term antifungal tablets (e.g. itraconazole or voriconazole)
⚠️ 2. Chronic Fibrosing Pulmonary Aspergillosis (CFPA)
Advanced stage of CPA
-
Happens when long-term infection causes lung scarring (fibrosis)
-
Lungs become stiff, making breathing harder
Symptoms:
-
Worsening breathlessness
-
Low oxygen levels
-
Severe fatigue
Treatment: Focuses on antifungals, symptom relief, and oxygen if needed
🟢 3. Simple Aspergilloma
A single fungal ball in a lung cavity
-
A round ball of fungus (aspergilloma) forms in an existing lung cavity
-
Often found during scans done for other reasons
-
Some people have no symptoms at all
Main risk: Coughing up blood (sometimes serious)
Treatment:
-
Monitoring if mild
-
Surgery or embolisation if bleeding occurs
🔴 4. Subacute Invasive Aspergillosis (SAIA or CNPA)
Faster-moving form of CPA
-
Occurs over weeks to months
-
Often seen in people with weaker immune systems (e.g. due to diabetes, steroids, or alcohol dependence)
-
Infection starts to invade deeper lung tissue
Symptoms:
-
Fever
-
Worsening breathlessness
-
Severe weight loss
Treatment: Prompt antifungal treatment and close medical monitoring
🟡 5. Aspergillus Nodules
Small lumps caused by Aspergillus
-
These are solid nodules in the lungs, often found by chance on a CT scan
-
They may be mistaken for cancer at first
-
Often cause no symptoms
Treatment:
-
Usually watch and wait
-
Sometimes surgery or biopsy if uncertain
🩺 Why Knowing Your CPA Type Matters
Understanding your CPA type helps your medical team:
-
Choose the best treatment for you
-
Monitor for bleeding or lung damage
-
Decide when to repeat scans or adjust medication
💬 Questions to Ask Your Doctor
-
Which type of CPA do I have?
-
Will I need long-term antifungal treatment?
-
How often should I have scans or blood tests?
-
What should I do if I cough up blood?
🧘 Final Note
CPA is a chronic condition, but many people manage it well with the right treatment and regular check-ups. You are not alone — support and information are available.
🏥 Surgery in Patients with ABPA or CPA: Can It Worsen Symptoms, and Should It Proceed?
Patients with Aspergillus-related lung diseases, such as Allergic Bronchopulmonary Aspergillosis (ABPA) and Chronic Pulmonary Aspergillosis (CPA), sometimes report worsened symptoms after undergoing surgery under general anaesthetic. While this is a recognised clinical pattern, it does not mean surgery should be avoided. Instead, it requires preparation and close perioperative management to reduce risk.
🔍 Can Surgery Worsen Aspergillosis Symptoms?
Yes — and here's why:
✳️ 1. Airway Irritation from Intubation
-
Endotracheal tubes can irritate airways already inflamed by ABPA or structurally altered by CPA.
-
Mechanical ventilation can impair mucus clearance and exacerbate cough or infection.
✳️ 2. Postoperative Immunosuppression
-
Surgery temporarily suppresses immune function.
-
Perioperative corticosteroids or stress-induced immune suppression can permit fungal flare-ups or reactivation.
✳️ 3. Impaired Mucus Clearance
-
Pain, immobility, and sedation reduce the patient’s ability to cough and clear secretions.
-
In CPA or ABPA, this can lead to plugging, fungal regrowth, or secondary bacterial infection.
✳️ 4. Drug Interactions
-
Azole antifungals (e.g. itraconazole, posaconazole) interact with many anaesthetics, opioids, and steroids.
-
These interactions can alter drug levels, reduce antifungal efficacy, or increase toxicity risk.
✳️ 5. Stress and Inflammation
-
Surgical stress may worsen the inflammatory or allergic component of ABPA.
-
CPA-related cavities may bleed or become re-infected post-op.
✅ Should Surgery Still Go Ahead?
Yes — surgery can and often should proceed when it is medically indicated.
Delaying needed procedures (e.g. for cancer, fractures, or pain relief) can lead to worse outcomes than the potential risks related to aspergillosis.
🛡️ Recommended Precautions
🔷 Pre-Operative Planning
-
Ensure all care teams are aware of the diagnosis.
-
Review lung imaging, baseline oxygenation, and current antifungal/steroid regimens.
-
Arrange for pre-op airway clearance if sputum is a concern.
🔷 Antifungal Management
-
Continue antifungal therapy through the perioperative period.
-
Use IV formulations if oral administration isn’t possible.
-
Check for drug interactions with anaesthetic or post-op medications.
🔷 Steroid Cover (ABPA and CPA on steroids)
-
Patients on chronic steroids may need perioperative hydrocortisone supplementation (adrenal cover).
-
Apply “sick day rules” or use the patient’s adrenal insufficiency plan, if applicable.
🔷 Post-Op Monitoring
Watch for:
-
Worsening cough, breathlessness, or sputum
-
Fever or signs of secondary infection
-
Raised IgE (in ABPA) or haemoptysis (in CPA)
-
Any signs of antifungal failure or drug toxicity
⚠️ When Might Surgery Be Delayed?
Consider postponing non-urgent surgery if:
-
There is active haemoptysis
-
The patient has uncontrolled inflammation or fungal burden
-
A recent scan shows expanding cavities or new infiltrates
-
Antifungal resistance is suspected or not yet managed
💬 Key Message for Patients
“Having ABPA or CPA doesn’t mean you can’t have surgery — but we do need to take extra care around your airways, your antifungal treatment, and your recovery. With the right team and planning, we can safely support you through your procedure.”

Allergic Bronchopulmonary Aspergillosis (ABPA) Without Asthma: A Hidden Reality
Most people – including many doctors – associate Allergic Bronchopulmonary Aspergillosis (ABPA) almost exclusively with asthma or cystic fibrosis. In fact, the current diagnostic criteria for ABPA often assume the presence of asthma as a prerequisite. But what happens when a patient has all the features of ABPA… without ever having had asthma?
This article explores the possibility – and growing recognition – of ABPA without asthma.
🔍 What Is ABPA?
ABPA is an allergic (hypersensitivity) reaction to the fungus Aspergillus fumigatus, which can colonise the lungs and cause:
-
Severe allergic inflammation
-
Damage to lung tissue (bronchiectasis)
-
High levels of IgE (often >1000 IU/mL)
-
Positive skin tests or blood tests for Aspergillus
Traditionally, ABPA is diagnosed in people with asthma or cystic fibrosis, where the airways are already vulnerable.
❗But Can ABPA Occur Without Asthma?
Yes. Though uncommon, there are confirmed cases where ABPA occurs in people who:
-
Do not have asthma
-
Have no wheeze, breathlessness or variability in symptoms
-
Show no reversibility on a bronchodilator test
-
May not respond to inhaled corticosteroids
This presentation is now increasingly recognised – particularly:
-
After viral infections like COVID-19
-
In people exposed to environmental moulds
-
In those with no personal or family history of asthma
🧪 Diagnostic Clues
Patients with ABPA but no asthma typically still show:
-
Very high total IgE levels
-
Positive Aspergillus-specific IgE and IgG
-
Radiological changes like central bronchiectasis
-
Sometimes eosinophilia in blood
But they do not show:
-
Classic asthma symptoms (e.g. wheeze, reversible breathlessness)
-
Improvement with bronchodilators
-
Variable peak flow readings
🧬 How Might This Happen?
There are a few theories:
-
Some people have a strong allergic immune response (IgE-driven) to Aspergillus alone, even without underlying asthma
-
COVID-19 and other infections may prime the immune system or damage airways enough to allow fungal colonisation
-
Not all bronchial hypersensitivity is asthma — the airway inflammation in ABPA is unique and not always “asthmatic” in pattern
✅ What Tests Can Help Confirm or Rule Out Asthma?
For patients who have ABPA but no clear asthma symptoms:
-
Bronchodilator reversibility test → May be negative
-
Methacholine or histamine challenge test → Gold standard for confirming asthma
-
FeNO test → Measures eosinophilic airway inflammation (may be high in both ABPA and asthma)
-
Peak flow monitoring → Often stable in ABPA without asthma
These tests can help clarify the diagnosis and prevent mislabeling patients as asthmatic when they are not.
🧭 Why Does It Matter?
Correct diagnosis matters because:
-
Not all ABPA patients benefit from inhaled corticosteroids or asthma drugs
-
Treatment should be tailored — e.g. antifungals and oral steroids for ABPA, but not unnecessary asthma medications
-
Misdiagnosis may delay the right treatment and overburden patients
🩺 A Call to Clinicians
If a patient has high IgE, bronchiectasis, and strong Aspergillus sensitisation — but no clinical asthma — consider ABPA without asthma.
Request confirmatory tests before labeling someone asthmatic for life. In these rare cases, asthma criteria do not fully apply — but the patient still needs support for ABPA.
🧾 Summary
| Feature | ABPA With Asthma | ABPA Without Asthma |
|---|---|---|
| Wheeze/breathlessness | Common | May be absent |
| Bronchodilator response | Often positive | Usually negative |
| Total IgE | High | High |
| Aspergillus IgE/IgG | Positive | Positive |
| Imaging (HRCT) | Bronchiectasis | Bronchiectasis |
🙋 What Can Patients Do?
If you’ve been diagnosed with ABPA but don’t believe you have asthma:
-
Ask your doctor about further testing to confirm or rule out asthma
-
Keep a record of your symptoms, peak flow (if used), and medication response
-
Discuss your IgE levels, CT scan results, and whether other diagnoses (e.g. chronic pulmonary aspergillosis) might apply
Adrenal Insufficiency in Aspergillosis: Important Risks for Patients and GPs

🫁 Who is at Risk?
People with aspergillosis — especially ABPA (Allergic Bronchopulmonary Aspergillosis) and CPA (Chronic Pulmonary Aspergillosis) — are often treated with:
- Steroids (inhaled or oral, such as fluticasone or prednisolone)
- Azole antifungal medications (like itraconazole, voriconazole, posaconazole)
Both of these can affect the adrenal glands, though azole antifungals only do so indirectly in combination with a steroid medication. When used together, or when steroids are used on their own for long periods of time at a high dose, they can significantly increase the risk of a serious condition called adrenal insufficiency (AI) — when the body can’t produce enough cortisol to respond to stress or illness.
💊 Why Azole Antifungals Make This Worse
Azoles (itraconazole, voriconazole, posaconazole) block liver enzymes (CYP3A4) that normally break down inhaled or oral steroids. As a result:
- Even inhaled steroids (like fluticasone or budesonide) can build up in the body
This can lead to systemic steroid effects, including:
- Adrenal suppression
- Cushing’s-like symptoms (weight gain, moon face, skin thinning)
- Higher risk of adrenal crisis if steroids are stopped too fast or during illness
This is especially well documented with fluticasone + itraconazole — a known high-risk combination.
🚨 What is Adrenal Insufficiency?
Adrenal insufficiency means your adrenal glands cannot produce enough cortisol, the hormone your body needs to:
- Regulate blood pressure and sugar
- Respond to infections and illness
- Maintain energy, mood, and salt balance
Without cortisol, even a minor illness can become life-threatening — this is called an adrenal crisis.
🔍 Warning Signs of Adrenal Suppression
- Fatigue and muscle weakness
- Low mood or confusion
- Weight loss or loss of appetite
- Dizziness when standing (low blood pressure)
- Nausea, abdominal pain
- Skin changes (e.g. thin skin, stretch marks, bruising)
- Cushingoid appearance (round face, fat on upper back)
- During stress (infection, surgery, trauma), people may:
- Vomit or collapse
- Become drowsy or disoriented
- Experience dangerously low blood pressure or blood sugar
🛡️ What GPs and Patients Should Do
For GPs:
- Be alert to the interaction between inhaled corticosteroids and azoles
- If a patient is using inhaled fluticasone or budesonide and starts azoles:
- Consider switching to a non-CYP3A4-metabolised inhaler (e.g. beclometasone)
- Monitor for signs of adrenal suppression or Cushing’s
- If adrenal insufficiency is suspected:
- Arrange morning cortisol testing
- Consider Short Synacthen Test (SST)
- Educate patients on sick day rules and ensure:
- A steroid emergency card is provided
- An adrenal crisis plan is in place
- Emergency hydrocortisone is prescribed if needed
For Patients:
Tell your GP or specialist if you are on:
-
- Azoles (like itraconazole, posaconazole)
- Any form of steroids (inhaled, nasal, oral, injected)
- Never stop steroids suddenly — they may need to be reduced slowly
- Report symptoms like fatigue, nausea, or dizziness
- Ask about a sick day plan — you may need to double your steroid dose during illness
- If you become very unwell, tell emergency services you are at risk of adrenal crisis
💬 Summary
Adrenal insufficiency is a real and under-recognised risk in aspergillosis — especially when azole antifungals are used alongside inhaled or oral steroids. Patients and GPs should work together to prevent and manage this serious complication.