
Working With Your Medical Team: What Every Patient With Aspergillosis Needs to Know
Modern antifungal treatments, and many of the medicines used alongside them, can be life-saving. They help control infections that would otherwise cause severe damage to the lungs and other organs. But these medicines are also powerful, and like all strong treatments, they sometimes carry risks.
One patient recently shared that they developed nerve damage (neuropathy) while taking antifungal medication, but did not mention it to their doctor because they did not know it could be a side effect. Sadly, problems like this can sometimes become permanent if not spotted early.
This raises an important question: what do patients need to know about their responsibilities when taking medicines like antifungals, and more broadly, when living with aspergillosis?
From passive role to partnership
In the past, healthcare often worked in one direction: the doctor gave instructions, and the patient was expected to follow them. Patients were mostly passive, with little chance to ask questions or take part in decisions.
The NHS is now moving towards a very different way of working: partnership.
This means:
-
Doctors and nurses share their medical knowledge.
-
Patients share their experiences of living with their condition.
-
Together, both sides decide what treatment and care will work best.
Why doctors sometimes hesitate about side effects
Some patients are surprised to learn that not all doctors automatically tell patients about possible side effects. Why is this?
-
Some worry about causing anxiety or putting patients off treatment.
-
Others fear the nocebo effect — where simply knowing about a side effect can make someone more likely to notice it.
-
They may also feel that handing over a long list of possible effects is overwhelming.
But when it comes to antifungals and other long-term, powerful medicines, not knowing can be dangerous. If patients do not know what to look for, they may ignore early signs of serious problems until it is too late.
The best approach is balance:
-
Patients don’t need to memorise an endless list.
-
They do need a clear, short list of the most important and urgent symptoms to look out for — and to know what to do if they appear.
Medicines: what patients should do
-
Take medicines as prescribed – antifungals, inhalers, steroids, or biologics must be taken on schedule. Missing doses can reduce effectiveness or drive resistance.
-
Do not stop suddenly – especially steroids. Always follow tapering advice.
-
Check for interactions – antifungals can clash with common medicines such as statins, blood pressure tablets, and painkillers. Always tell your team about new prescriptions, over-the-counter drugs, or supplements.
-
Use the same pharmacy if possible – so interactions are checked consistently.
Monitoring your health
-
Attend all scheduled tests – blood work, lung function, CT scans. These can reveal hidden changes before you feel them.
-
Know your “normal” – keep track of oxygen levels (if you use a pulse oximeter), peak flow, sputum colour, cough, and breathlessness.
-
Spot infections early – worsening cough, fever, or new sputum colour may mean infection or flare-up. Report these quickly.
Communication with your team
-
Bring notes to clinic – write down questions and symptoms so nothing is forgotten.
-
Be open and honest – if you’ve missed doses, struggled with side effects, or found treatment difficult, let your team know.
-
Keep contact details handy – know who to call if problems arise (specialist nurse, hospital helpline, GP).
Lifestyle and prevention
-
Reduce exposure to moulds – avoid compost heaps, rotting leaves, damp basements, and building dust. If you cannot avoid them, wear an FFP2/3 mask.
-
Protect your lungs – keep up with vaccinations (flu, COVID-19, pneumococcal).
-
Support your overall health – eat well, stay as active as you can, and rest when needed.
-
Look after your mental health – chronic illness is stressful. Patient groups, counselling, or peer support can make a big difference.
Self-management skills
-
Recognise flare-ups – learn the difference between ABPA flare, CPA progression, and bacterial infection symptoms.
-
Know your rescue plan – what to do if you suddenly worsen (extra inhalers, antibiotics, or emergency help).
-
Keep records – note symptoms, hospital visits, and medication changes. This helps spot long-term patterns.
-
Be part of decisions – ask about benefits, risks, and alternatives of treatments. Care should fit your life as well as your lungs.
Where to find reliable information on medicines
Many patients say the leaflet in the medicine box is written in tiny print or feels overwhelming. You do have other options:
-
Ask your clinical team or pharmacist — they can give you a short list of the most important side effects to watch for and explain what’s urgent.
-
Check the BNF (British National Formulary) online — the NHS makes this trusted reference free to the public at bnf.nice.org.uk. It lists side effects, drug:drug interactions, and safety notes.
-
Use NHS.uk — clear pages on most medicines, written in plain English.
-
Patient support organisations — such as the National Aspergillosis Centre or relevant charities, which often provide tailored advice.
If you’re unsure, it’s always safer to ask rather than guess.
The bigger picture: partnership
In the past, doctors made decisions and patients followed instructions. Today, with complex conditions like aspergillosis, patients are central members of the care team.
-
You notice problems first.
-
You take daily responsibility for medication.
-
You decide when to seek help.
This isn’t about shifting the whole burden onto patients — it’s about recognising that care works best when it is a true partnership.
Key message
👉 If you notice something new, strange, or worrying while on antifungal medication — however small — tell your healthcare team. Don’t assume it’s not important.
And remember: safe, effective treatment is a two-way street. Your role as a patient is not just to take medicines, but to observe, record, communicate, and partner with your team. That partnership is what keeps you safe and makes your treatment work.
Misinformation on Social Media: Health and Beyond
Social media helps us stay connected, share experiences, and find support. But it also spreads false or misleading stories — about health, politics, money, and world events. These stories can cause unnecessary fear, confusion, and sometimes real harm if people act on them.
Understanding why misinformation spreads, what’s being done about it, and how to spot it helps keep you and your loved ones safe.
🚩 Why do false stories spread?
-
Algorithms reward attention
Platforms are designed to keep you scrolling. Content that shocks (“miracle cure discovered!”), scares (“hidden danger you’re not being told about!”), or excites spreads the fastest — even if it isn’t true. -
Anyone can post anything
Unlike newspapers, medical journals, or BBC/NHS websites, most social media posts aren’t checked by editors or experts before going live. -
Echo chambers
Platforms show you more of what you already click on. If you read about miracle diets or political conspiracies, you’ll see more of them — true or not. -
Deliberate misinformation
Some people spread falsehoods deliberately:-
To sell fake health products
-
To make money from clicks
-
To influence politics or sow division
-
-
Speed beats accuracy
False stories can go viral in minutes. Corrections are slower and rarely reach as many people.
⚖️ What’s being done about it?
Legal approaches
-
UK: The Online Safety Act (2023) requires platforms to remove illegal or harmful misinformation, including dangerous health advice.
-
EU: The Digital Services Act (DSA) makes large platforms responsible for acting faster against harmful content.
-
Extreme cases: Fraud, scams, defamation, or incitement of violence are not protected speech and can be prosecuted.
Technical approaches
-
Algorithms: AI flags suspicious posts.
-
Labelling: Content can be marked as “false” or “missing context.”
-
Bot control: Platforms limit fake accounts that spread stories at scale.
-
Digital nudges: Some apps ask “Do you want to read before sharing?” or warn if a post is outdated.
The limits
-
Freedom of speech protects many misleading opinions unless they cause direct harm.
-
Global reach makes it hard to police.
-
Volume — billions of posts daily are impossible to check one by one.
-
Trust — some people ignore fact-check labels, believing platforms are biased.
🧐 How to know what’s real
Five quick checks:
-
Who is posting it? NHS, WHO, BBC, or Reuters → reliable. Unknown influencer or “miracle cure” shop → beware.
-
Is it reported elsewhere? Real news appears in multiple reputable outlets.
-
Does it use scare tactics or hype? “Doctors don’t want you to know this secret cure!” → red flag.
-
Can you fact-check it? Try NHS.uk, Full Fact (UK), Snopes, Reuters Fact Check or BBC Verify.
-
Check dates and pictures — old or unrelated content is often recycled to look new.
🚦 The traffic-light test
-
🟢 Green – from official sources, confirmed, calm tone → likely true.
-
🟡 Amber – source unclear, dramatic style, no confirmation elsewhere → pause, check.
-
🔴 Red – sensational, “miracle” claims, conspiracy, or urging you to share → almost certainly false.
💡 Should we avoid social media completely?
Not necessarily. Social media has real value for support, awareness, and connection. The key is using it wisely:
-
Follow trusted organisations for health and news.
-
Unfollow or mute accounts that regularly spread falsehoods.
-
Balance social media with direct trusted sources (NHS, GP, recognised news).
-
Step away if scrolling leaves you anxious, angry, or confused.
✨ Bottom line
False stories spread online because the system rewards attention, not accuracy. Laws and technology help, but they can’t stop misinformation entirely.
The best defence is awareness. Before acting on or sharing any post — whether about health, politics, or world events — pause, check, and if in doubt, don’t share.
👉 Protecting yourself from misinformation means protecting your community too.
📚 New Children’s Book Helps Families Understand Aspergillosis
Launch Event at Affinity Outlet, Fleetwood – 13th September 2025
The Aspergillosis Trust is delighted to announce the launch of a brand-new children’s book, Dad and the Sneaky Spores, written by award-winning author Christina Gabbitas and beautifully illustrated by Ursula Hurst.
This story has been specially commissioned to raise awareness of aspergillosis, a serious lung condition caused by the Aspergillus fungus. Through gentle storytelling and colourful illustrations, the book helps children and families understand what it means to live with a parent affected by aspergillosis.
✨ About the Event
📅 Date: Saturday 13th September 2025
📍 Location: Affinity Outlet, Fleetwood
The launch event will be a fun and informative day for all the family.
-
✍️ Meet the Author: Christina Gabbitas will be signing copies of the book between 12pm and 2pm.
-
👩⚕️ Ask the Experts: A qualified nurse will be available to answer medical questions or offer advice.
-
📚 Learn Together: Families can explore how storytelling can make complex health conditions easier to understand.
📖 About Dad and the Sneaky Spores
The book follows a family’s journey with aspergillosis in a way that children can relate to. It not only explains the illness but also encourages empathy, resilience, and understanding within families.
“The narrative not only educates readers about aspergillosis but is also thoughtfully crafted to foster empathy and understanding.” – Aspergillosis Trust
Published by Poems & Pictures, Dad and the Sneaky Spores is available from 1st August 2025.
💜 Why This Matters
Aspergillosis is a rare and often misunderstood condition. By raising awareness through creative storytelling, this initiative provides a new way to start important conversations with children, families, and the wider community.
🔗 Find out more at: www.aspergillosistrust.org

NHS England - You and Your GP: Key Points for NHS Patients Managing Aspergillosis
You and your general practice (YYGP) has been developed to help patients understand what to expect from their general practice and how they can get the best from their GP team. YYGP also enables patient to provide feedback or raise concerns with their GP Practice, Healthwatch or the integrated care board. The contract requires every GP practice to have linked to the NHS England YYGP document on their website, no later than 1 October 2025.
1. Accessing Your GP
-
Opening hours: Your GP is typically open 8:00 – 18:30, Monday to Friday. You can walk in, call, or use the NHS App or practice website to contact them NHS England.
-
If closed: For urgent but non-emergency needs, use 111 online or by calling 111 NHS England.
-
In an emergency: If symptoms are life-threatening (e.g., sudden severe breathing issues), go to A&E or call 999 NHS England.
2. Making an Appointment
-
When you contact your GP—whether by phone, online, or in person—they’ll assess your condition and respond within one working day with next steps NHS England.
-
This could include:
-
A face-to-face appointment
-
A phone consultation
-
A text message with advice
-
A recommendation to consult a pharmacy or another NHS service NHS England.
-
This prompt response is especially important for aspergillosis fluctuations or side effects from antifungal treatments.
3. Who You'll See
-
You may be seen by a GP, nurse, or pharmacist.
-
If you have a designated carer, they can speak on your behalf (with your permission).
-
If you prefer a specific healthcare professional you trust, request them—though waits might be longer NHS England.
-
Seeing the same clinician regularly can be beneficial for managing complex, long-term conditions like aspergillosis NHS England.
4. Support for Additional Needs
-
If English isn't your first language, you can request interpretation services when booking an appointment.
-
If you need extra help—like longer appointments, a quiet space, wheelchair access, or materials in accessible formats—just let the practice know; they'll try to accommodate NHS England.
5. Changing or Selecting a GP
-
You can find or switch to a GP using the NHS website (“Find a GP”) or by contacting local practices directly NHS England.
-
No ID, NHS number, or proof of address is needed to register—even if you’re homeless or your immigration status is uncertain NHS England.
-
If a practice cannot register you, they must explain their decision in writing within 14 days NHS England.
6. Referral and Treatment Flexibility
-
If your GP refers you to a specialist (e.g., respiratory consultant), you often have the right to choose your hospital or clinic NHS England.
7. Free Care & Private Work
-
GP services are free, including appointments and treatments.
-
Extra services like insurance letters may incur a fee NHS England.
8. Being a Helpful Patient
-
Prepare for appointments: list symptoms, treatment concerns, and questions in advance.
-
Be punctual or cancel in good time to avoid delays for others.
-
Use the NHS App or website to book appointments, refill prescriptions, and view test results.
-
Turn on App notifications to stay updated with messages from your practice NHS England.
-
Order repeat prescriptions well ahead—especially vital when managing antifungal medications—to avoid running out NHS England.
-
Consider joining the Patient Participation Group at your practice to share feedback and help improve services NHS England.
9. Sharing Feedback or Concerns
-
To raise concerns, talk to your practice manager first.
-
If needed, you can escalate feedback to your local Integrated Care Board (ICB).
-
You can also reach out to your local Healthwatch (an independent NHS watchdog) for confidential advice and support NHS England.
Why This Matters for Aspergillosis Patients
Aspergillosis often requires ongoing monitoring, regular breathing tests, imaging, and antifungal therapy adjustments. Timely access to GP services, continuity of care, and preparedness all enhance your ability to manage flare-ups or side effects effectively.
Handy Checklist (for easy reference)
| Task |
|---|
| Contact GP promptly for new or worsening symptoms |
| Prepare questions ahead—e.g., changes in breathing, treatment effects |
| Use NHS App to manage appointments and medications |
| Order repeat prescriptions early to maintain drug access |
| Request support services if needed (interpretation, accessibility) |
| Provide feedback to improve your experience and others' |

Shared Care Records in the NHS: What Aspergillosis Patients Need to Know
The NHS is changing how patient records are managed. By 2026, every area of England will have a Shared Care Record. This is not one big “national record,” but a way of securely linking together the different records held by your GP, hospital, and other services.
For patients with aspergillosis, this could make a real difference to care, safety, and research.
🗂 What Is a Shared Care Record?
-
Not one single file: Your GP, hospital, and community services keep their own systems.
-
Linked together: Clinicians can securely view a joined-up picture of your health.
-
Safer and faster care: Your allergies, test results, and medications can be seen wherever you are treated.
-
You tell your story once: No more repeating details every time you see a new doctor.
🛡 How Safe Is My Data?
-
Strict access control: Only staff directly involved in your care can open your record.
-
Audit trail: Every time it’s viewed, the system records who, when, and why.
-
Encryption & firewalls: Records are locked against outside access.
-
No mass downloads: Systems only allow one patient’s record at a time.
In many ways, this is safer than old paper notes, which could be lost, copied, or seen by accident.
👩⚕️ Confidentiality Rules Stay the Same
-
NHS staff are bound by confidentiality laws and the Caldicott Principles.
-
Looking at a record without a valid care reason is a disciplinary offence.
-
Your record is not shared with insurers, employers, or relatives without your consent.
📊 Research and Aspergillosis
Shared Care Records could also help improve research into aspergillosis, which is often under-recognised:
-
Better case finding: Linking GP, hospital, and lab data makes it easier to identify true cases.
-
Tracking outcomes: Researchers can follow IgE/IgG results, CT changes, and treatment responses over time.
-
Environmental links: Data could be combined with housing, air quality, and weather information.
-
Support for trials: Easier to find eligible patients for new antifungal or biologic studies.
All research use is usually de-identified (your name and personal details removed). You can choose to opt out via the National Data Opt-Out if you don’t want your data used in this way.
🏦 Will Insurance Companies See My Record?
No. Insurance companies and employers cannot access your NHS record.
If you apply for insurance, your GP may be asked for a report — but this is only done with your consent.
🌐 What If I Don’t Use the Internet?
You don’t need to be online to benefit. Shared Care Records are mainly for clinicians, not for patients logging in.
If you want to see your record, you can still ask for a paper copy from your GP or hospital.
📍 Who Runs Shared Care Records?
They are organised locally by Integrated Care Systems (ICSs).
-
England is divided into 42 ICSs, each bringing together NHS services, local councils, and community care.
-
Examples include Greater Manchester ICS, Cheshire & Merseyside ICS, and North East London ICS.
-
Scotland, Wales, and Northern Ireland use different systems.
✅ Key Reassurances for Patients with Aspergillosis
-
Your data remains confidential and secure.
-
Shared Care Records mean joined-up, safer care across GP, hospital, and community services.
-
Insurers and employers cannot access your NHS record.
-
You stay in control — you can opt out of data use for research if you wish.
-
The new system could help advance aspergillosis research, leading to better diagnosis and treatments.
🩺 NHS Data Sharing: How It Will Improve Your Care
🌍 The Problem Today
At the moment, your health information is stored in many different places:
-
Your GP (General Practitioner) has one record.
-
Hospitals keep their own records.
-
Community services (like district nurses or physiotherapists) have separate notes.
-
Social care also keeps its own information.
This can cause problems:
-
You may be asked to repeat your story again and again.
-
Doctors don’t always see the full picture (medications, allergies, past test results).
-
Sometimes tests are repeated unnecessarily.
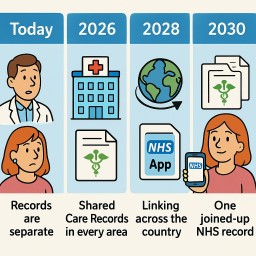
📅 The Timeline for Change
Today (2025)
-
Records are mostly separate.
-
Some areas already share basic information like your medicines and allergies through a “Summary Care Record.”
👉 What it means for you: You still have to repeat information at most appointments.
2026 – Shared Care Records in Every Area
-
Every region (called an Integrated Care System, or ICS) will have a Shared Care Record.
-
This links together information from GPs, hospitals, community teams, and social care.
-
Hospitals using modern systems like Epic (a type of electronic patient record - MFT has installed this already) can also start sharing directly with other Epic hospitals.
👉 What it means for you: Doctors can see more of your health record without asking you to repeat everything.
2028 – Linking Across the Country
-
Regional Shared Care Records will start to connect with each other.
-
Epic hospitals across the UK will share records more easily using Care Everywhere (Epic’s sharing tool).
-
Community services and “virtual wards” (hospital care at home) will be fully connected.
👉 What it means for you: If you are treated in another part of the country, staff there will be able to see important parts of your health record straight away.
2030 – One Joined-Up NHS Record
-
The NHS plans to give every patient a longitudinal record – one joined-up health and care record that follows you everywhere.
-
This will combine information from GPs, hospitals, community services, mental health teams, and social care.
-
Patients will also be able to see much more of their own record through the NHS App.
👉 What it means for you: Wherever you go in the NHS, staff can see your medical history safely. You’ll feel your care is joined-up, and you can also check your record yourself.
✅ Your Patient Journey: Step by Step
-
Today: “I have to explain my medication list every time. I’m not sure my hospital knows what my GP prescribed.”
-
2026: “When I go into hospital, the doctor can already see my GP record and community nurse notes.”
-
2028: “I was treated far from home, and the hospital could see my recent test results straight away.”
-
2030: “Wherever I go, the NHS staff have the full picture. I can see my record too on the NHS App.”

Damp, Cold, and Poor Housing – Why It Matters for Lung Health
This briefing from the House of Commons Library (2025) looks at how poor housing conditions—especially damp, mould, and cold homes—affect health and what’s being done about it in the UK.
Main Points
-
Health risks are serious
Living in damp or mouldy homes increases the risk of respiratory problems, particularly for people with existing lung disease like aspergillosis, asthma, COPD, or bronchiectasis. -
Children and vulnerable adults
Young children, older adults, and people with weakened immune systems are most affected. Damp and mould can trigger flare-ups, worsen breathing symptoms, and increase infection risk. -
Mental health impact
Poor housing is linked to stress, anxiety, and depression. Worrying about your home can also worsen physical symptoms, especially if you avoid using rooms with mould or limit heating to save costs. -
Cold homes add to the problem
Cold airways can make breathing more difficult, weaken the immune system, and increase the chance of winter infections. -
Wider health effects
Damp and cold can also affect heart health, bone/joint pain, and overall wellbeing.
What’s Being Done
-
Legal responsibilities: Landlords must keep homes safe and fit to live in under UK law. This includes dealing with serious damp and mould.
-
Government programmes:
-
Funding for improving insulation and heating in social housing.
-
Advice services for tenants.
-
Local councils can take action if landlords fail to address hazards.
-
-
Public health guidance now recognises the link between housing and chronic illness, with stronger advice for early intervention.
What This Means for Aspergillosis Patients
-
Stay alert to symptoms: If your cough, breathlessness, or fatigue worsen at home, check for damp, mould, or poor heating.
-
Act early: Report problems to your landlord or council quickly—prolonged exposure can worsen lung damage.
-
Medical link is recognised: You are more likely to be taken seriously now, as official guidance acknowledges the health risks.
-
Keep records: Photos, symptom diaries, and GP notes can support housing complaints.
For full details see https://commonslibrary.parliament.uk/research-briefings/cdp-2025-0096/
📘 What is CPA? (Chronic Pulmonary Aspergillosis)
Patient handout for A&E staff who are not aware of aspergillosis.
What is CPA?
CPA is a chronic fungal infection of the lungs caused by Aspergillus, most often in people who already have damaged lungs from conditions like tuberculosis, COPD, lung cancer, or sarcoidosis.
Unlike ABPA, CPA is a true infection, not an allergic reaction. It is not contagious but can slowly destroy lung tissue if not treated.
Symptoms
-
Chronic cough, often with mucus
-
Coughing up blood (haemoptysis)
-
Fatigue, low-grade fever
-
Unexplained weight loss
-
Breathlessness
-
Recurrent chest infections not responding to antibiotics
Diagnosis
-
CT scan of the chest showing cavities, nodules, or fungus balls (aspergillomas)
-
Aspergillus IgG antibody (usually raised)
-
Positive sputum PCR or culture for Aspergillus
-
Exclude TB and malignancy
Treatment
-
Long-term antifungal therapy (e.g. itraconazole, voriconazole, posaconazole)
-
Monitor blood levels and liver function
-
Surgery or embolisation if severe bleeding occurs
-
Supportive care: oxygen, nutrition, physiotherapy
Key Points for A&E:
✅ CPA is a progressive fungal infection, not a typical bacterial pneumonia
✅ May present with haemoptysis, respiratory distress, or systemic illness
✅ Review current antifungal treatment and potential drug interactions
✅ Consider urgent chest CT and specialist referral if patient is unwell
📍 For specialist support:
National Aspergillosis Centre (NAC)
🏥 Wythenshawe Hospital, Manchester University NHS Foundation Trust
🌐 NAC homepage on MFT website https://mft.nhs.uk/wythenshawe/services/infectious-diseases/national-aspergillosis-centre/
🌐 www.aspergillosis.org
📞 Daytime contact: 0161 291 2891 or 0161 291 4362
📞 Urgent out-of-hours: Call Wythenshawe switchboard on 0161 998 7070
📢 Ask for the on-call Infectious Diseases Consultant
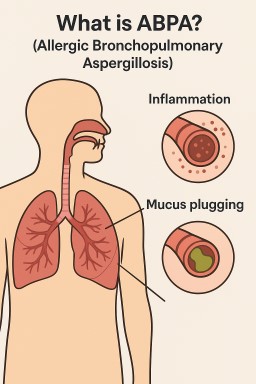
📘 What is ABPA? (Allergic Bronchopulmonary Aspergillosis)
Patient handout for A&E staff who ask what aspergillosis is.
What is ABPA?
ABPA is an allergic lung condition caused by the immune system overreacting to the fungus Aspergillus. It mainly affects people with asthma or cystic fibrosis.
When Aspergillus spores are inhaled, most people clear them without issue. In ABPA, the immune system sees these spores as dangerous and mounts a strong inflammatory response. This leads to asthma-like symptoms, mucus plugging, and can result in permanent lung damage (bronchiectasis) if left untreated.
Symptoms
-
Worsening breathlessness
-
Wheezing, chest tightness
-
Coughing up thick, often brown mucus
-
Fever, fatigue, or feeling generally unwell
-
Unintentional weight loss (advanced cases)
Diagnosis
-
History of asthma or cystic fibrosis
-
High IgE levels and positive Aspergillus-specific IgE
-
Eosinophilia (raised white blood cells)
-
Sputum culture or PCR positive for Aspergillus
-
Chest imaging showing mucus plugging or bronchiectasis
Treatment
-
Oral corticosteroids (e.g. prednisolone) to reduce inflammation
-
Antifungal medication (e.g. itraconazole) to lower fungal burden
-
Biologic therapies (e.g. omalizumab or benralizumab) in some patients
-
Regular monitoring by respiratory or infectious diseases specialists
Key Points for A&E:
✅ ABPA is an allergic lung disease, not a classical infection
✅ Can present with severe asthma, mucus plugging, or type 2 respiratory failure
✅ Requires early recognition and often systemic steroids and antifungal therapy
✅ Take bloods (IgE, eosinophils, CRP), consider chest imaging, and review oxygen status
📍 For specialist support:
National Aspergillosis Centre (NAC)
🏥 Wythenshawe Hospital, Manchester University NHS Foundation Trust
🌐 NAC homepage on MFT website https://mft.nhs.uk/wythenshawe/services/infectious-diseases/national-aspergillosis-centre/
🌐 www.aspergillosis.org
📞 Daytime contact: 0161 291 2891 or 0161 291 4362
📞 Urgent out-of-hours: Call Wythenshawe switchboard on 0161 998 7070
📢 Ask for the on-call Infectious Diseases Consultant

🤐 Why It's Important Not to Share Your Clinical Trial Experience — Until It’s Over
If you have chronic pulmonary aspergillosis (CPA), you may be invited to take part in a clinical trial for a new antifungal medication like rezafungin. That’s exciting — and could help improve treatment for many people in future.
Naturally, people want to support each other by sharing experiences, especially in online support groups. But when it comes to clinical trials, there’s a really important reason why we shouldn’t talk about how we’re feeling while we’re still in the trial.
Here’s why.
🧪 What Are Clinical Trials For?
Clinical trials help doctors and researchers answer important questions like:
-
Does this new treatment work?
-
Is it better than the current treatment?
-
What side effects might it cause?
To get accurate answers, the trial needs to be fair and unbiased — meaning that personal expectations and outside influences shouldn’t affect how people report their symptoms or progress.
📣 The Problem With Sharing During a Trial
If you’re taking part in a trial and say something like:
“I feel great — this new drug is working for me!”
or
“This is making me feel worse than ever — don’t join!”
...other people may change how they think and feel based on your comment.
This is called bias. It can:
-
Make others expect the same good (or bad) result
-
Affect how people rate their own symptoms
-
Cause people to drop out or not join at all
-
Make the trial results less accurate or even unusable
Even well-meaning comments can damage the study, especially if the trial is small (like most CPA studies are).
🕵️♀️ What If It’s a Blinded Trial?
Some trials are "blinded", meaning you don’t know whether you're getting the new treatment or a standard one (or placebo).
But if people start guessing or posting:
“I’m sure I’m on the real drug — I feel amazing!”
...then other people might also guess, or feel disappointed — which again, affects how results are reported.
🚦When Is It Safe to Share?
💬 After the trial is over and the results are published, you can talk freely about your experience.
In fact, patient voices are vital at that stage — they help others understand what it’s like to be part of a trial and whether new treatments are helpful in real life.
💡 What You Can Say During the Trial
You can still help raise awareness without compromising the study. For example:
-
✅ “I’m taking part in a CPA trial – ask your doctor if you might be eligible.”
-
✅ “There’s a study on a new antifungal — here’s the link to the official trial page: clinicaltrials.gov/study/NCT06794554”
-
✅ “I’m proud to be contributing to research — happy to share my experience once the trial ends.”
Just don’t talk about how the treatment is affecting you until the trial is complete.
🙏 Why This Matters
By keeping quiet during the trial, you're:
-
Protecting the integrity of the study
-
Helping future patients get trustworthy answers
-
Supporting the research team who need clear, unbiased data
You’re not just taking part in a trial — you’re helping build evidence that others will depend on for years to come.
🧭 Summary
| ✅ Do | ❌ Don’t |
|---|---|
| Tell people a trial exists | Share how the treatment is affecting you |
| Encourage others to talk to their doctor | Post guesses about which drug you’re on |
| Wait until the trial ends to share experiences | Influence others to join based on your results |
If you're ever unsure, ask your clinical trial team or group moderator — they'll be glad to help. Your role in research is important, and your silence now is a powerful act of support for science, fairness, and future care.