
💙 Disability Verification and Support for People with Aspergillosis in the UK
Living with aspergillosis—whether it's chronic pulmonary aspergillosis (CPA), allergic bronchopulmonary aspergillosis (ABPA), or another form—can have a significant impact on daily life. Many people find that fatigue, breathlessness, medication side effects, and other long-term symptoms affect their ability to work, care for themselves, or maintain independence.
If your condition is affecting your daily activities, you may be entitled to disability support, financial help, or adjustments at work or home. This guide explains how to get your disability recognised and verified in the UK, who can help, and how this varies across age groups and types of disability.
✅ What Counts as a Disability?
Under the Equality Act 2010, a person is classed as disabled if they have:
“A physical or mental impairment that has a substantial and long-term negative effect on their ability to carry out normal day-to-day activities.”
Many people with aspergillosis meet this definition—especially if they experience breathlessness, fatigue, pain, or recurrent infections over months or years.
📋 How Can You Prove or Verify Your Disability?
There is no single "disability certificate" in the UK. Instead, different systems accept different types of evidence, depending on what support you are applying for.
1. Benefit Award Letters
These are the most commonly accepted form of disability evidence:
- Personal Independence Payment (PIP)
- Disability Living Allowance (DLA) (for under 16s)
- Attendance Allowance (for over State Pension age)
- Employment and Support Allowance (ESA) (Support Group)
- Industrial Injuries Disablement Benefit
Where to get it: Contact the DWP or check your online account for a copy of your award letter.
2. NHS Medical Letters
Ask your GP or consultant to write a letter that:
- Confirms your diagnosis (e.g. CPA, ABPA)
- Describes the symptoms and how they affect your daily life
- Explains any treatments you need (e.g. antifungals, oxygen, steroids)
- States any long-term prognosis or care needs
3. Blue Badge and Disabled Bus Pass
- Blue Badge: Available from your local council for parking needs
- Disabled Bus Pass: Also issued locally; often requires proof of benefits or medical need
4. Occupational Therapy Assessment
- NHS or council-based OTs can assess your ability to manage daily tasks and recommend adaptations or support.
- Access via GP or Adult Social Care team.
5. Workplace or Education Support
- Occupational Health assessments may recommend reasonable adjustments such as flexible hours, remote work, or cleaner air environments.
- You may be eligible for Access to Work grants.
6. PIP and Other Benefit Assessments
- Assessments focus on how your condition affects daily tasks like mobility, personal care, medication management, and communication.
🔢 Do We Get a Disability Percentage?
In the UK, disability is not usually measured as a percentage. Most systems use functional assessments or point-based scoring.
The Exception: Industrial Injuries Disablement Benefit (IIDB)
- Uses a percentage system based on the extent of permanent disablement from a work-related condition.
For Everyone Else:
- PIP, DLA, and ESA use points-based systems.
- Employers, schools, and councils assess need based on impact, not percentage.
🡥 Who Can Help You with Disability Assessment?
| Professional / Service | Role & When to Use |
|---|---|
| GP or Specialist Consultant | Confirm diagnosis and functional impact for letters and forms |
| Occupational Therapist (NHS) | Assess your ability to manage daily tasks, recommend home aids/adaptations |
| Occupational Health (Work) | Recommend workplace adjustments under Equality Act |
| Adult Social Care (Council) | Assess for care support and home adaptation funding |
| Citizens Advice / Disability Charities | Help with forms, appeals, and understanding your rights |
| National Aspergillosis Centre (NAC) | May provide supporting letters for housing or benefits if you're under their care |
👶 Children and Young People
Under 16
- Claim Disability Living Allowance (DLA)
- Apply for an Education, Health and Care Plan (EHCP) if they have learning or developmental needs
- Get support from social care and school SENCOs
Age 16–25
- Transition to PIP for disability benefits
- EHCP can continue to age 25 if still in education
- Access workplace/education adjustments and Access to Work
- Shift from Children’s Services to Adult Social Care at 18
👵 Older Adults (Typically Age 65+)
Attendance Allowance
- For care needs only (not mobility)
- Not means-tested
Care and Support Needs
- Request a Care Act assessment from local council
- May result in home care, adaptations, or care home funding
NHS Continuing Healthcare
- For those with severe, complex needs
- Fully funded by NHS; not means-tested
Blue Badge Scheme
- Still accessible based on breathlessness or mobility limitation
Carer Support
- Carer's Assessment available
- Access to Carer’s Allowance or respite care
🧠 Mental Illness and Long-Term Invisible Disabilities
Mental health conditions and other non-visible disabilities (e.g. chronic fatigue, fibromyalgia, autism, long COVID) are also recognised under the Equality Act if they are long-term and impact daily life.
Differences in Assessment
- Focus is on non-physical activities:
- Planning and following journeys
- Managing therapy or medication
- Social interaction
- Decision-making
Key Evidence
- GP letters
- Psychiatrist or psychologist reports
- Occupational therapy or carer evidence
Support Services
- Community mental health teams (CMHT)
- Crisis teams, counselling, and talking therapies
- Supported housing or assisted living
Reasonable Adjustments
- Flexible schedules, quiet spaces, remote work
- Mental health support plans at school, university, or work
Advocacy
- Mind, Rethink, Disability Rights UK, and VoiceAbility provide advocacy, appeals help, and representation
📚 Summary Table
| Area | Physical Disabilities | Mental Health / Invisible Disability | Children | Older Adults |
| Benefit | PIP / ESA | PIP / ESA | DLA | Attendance Allowance |
| Social Care | Adult Social Care assessment | Adult Social Care or MH services | Children’s Services | Adult Social Care |
| Education/Work Support | Access to Work, OH reports | Access to Work, reasonable adjustments | EHCP, SENCO | Retirement/flexible options |
| Blue Badge | Based on mobility | Based on anxiety/severe distress for travel | May be available | Common for respiratory limits |
| Evidence Needed | Consultant, OT, GP | Psychiatrist, GP, carer, advocate | School or paediatric reports | GP, consultant, OT |
| Advocacy Support | Citizens Advice, Scope | Mind, Rethink, Disability Rights UK | IPSEA, Contact | Age UK, Carers UK |
🙏 Final Tips
- Keep copies of all letters, forms, and award notices.
- If your condition fluctuates, keep a symptom diary to show variable impact.
- Apply for assessments early as processes can take time.
- If you need help applying, speak to Citizens Advice or a local disability advocacy service.
- The National Aspergillosis Centre may be able to support patients with evidence for housing, benefit, or support applications.

🫁 Mucus Plugging in Aspergillosis: What It Is, Why It Happens, and What It Means
For patients with ABPA, CPA, Aspergillus bronchitis, or asthma
🔍 What Is a Mucus Plug?
A mucus plug is a thick clump of sticky mucus that becomes trapped in your lungs. It can block airways, cause coughing, and make breathing more difficult. In people with aspergillosis, this is common — but the type, location, and cause of the mucus can vary.
🧪 What Causes Mucus Plugging?
Your lungs naturally make mucus to protect against germs and irritants. But in fungal or allergic lung disease, this mucus may:
-
Be produced in excess
-
Become too thick or sticky
-
Get trapped due to airway damage
Aspergillosis-related causes include:
-
ABPA (Allergic Bronchopulmonary Aspergillosis) – inflammation causes thick, sticky mucus
-
Aspergillus bronchitis – fungus lives in mucus, producing biofilms
-
CPA (Chronic Pulmonary Aspergillosis) – may lead to mucus due to structural damage
-
Bronchiectasis – airways are widened and can no longer clear mucus properly
🧬 Are All Mucus Plugs the Same?
No. Mucus plugs vary in colour, texture, cause, and treatment. Here's how they differ:
| Type of Plug | What You Might See | What It Could Mean | Common in... |
|---|---|---|---|
| Sticky, stringy | Clear/yellow, like glue | Allergic inflammation | ABPA, asthma |
| Rubbery or solid | Brown, rubbery, “slug-like” | Allergic + fungal mix | ABPA, Aspergillus bronchitis |
| Green or smelly | Thick, foul-smelling | Infection (bacteria) | Bronchiectasis |
| Foamy or frothy | Clear/white, bubbly | Non-infectious irritation | COPD, asthma |
| Black or speckled | May contain fungal specks | Fungal growth | CPA, fungal bronchitis |
🖼️ What Do Mucus Plugs Look Like on a CT Scan?
Below are real examples of CT scan findings showing mucus plugging in different forms of aspergillosis and related conditions.
🧷 1. Finger-in-glove sign (ABPA)
Mucus in large airways appears like fingers inside a glove. This is common in allergic fungal airway disease.
➡ Seen in: ABPA, bronchiectasis with fungal colonisation
📍 Note: Branching tubular opacities filled with mucus.
🌿 2. Tree-in-bud pattern
Small airway blockage — plugs in the tiniest branches of the lungs. Common in infection, inflammation, and Aspergillus bronchitis.
➡ Seen in: Aspergillus bronchitis, asthma, CPA with superinfection
📍 Note: Tiny dots and lines in a tree-like shape.
🧱 3. Lung collapse (atelectasis) from plug
A large mucus plug can block a main airway, causing collapse of part of the lung.
➡ Seen in: Severe ABPA, CPA, patients with weakened cough reflex
📍 Note: Whiteout of part of lung where plug is blocking airflow.
📸 Example CT Findings

1. Bronchiectasis + mucus plug
Area in the left lower lung shows dilated bronchi filled with mucus—classic for bronchiectasis with mucoid impaction

2. Extensive bronchiectasis with plugs
Widespread thick-walled airway dilatation accompanied by mucus plugs (black arrows) and consolidation (black arrowheads)

3. Luminal plugging in small airways
Subtle luminal opacities in peripheral bronchi—the “tree‑in‑bud” pattern common in asthma, COPD, and infections.

4. Atelectasis (part of the lung has collapsed or isn’t fully inflating) due to mucus plugging
Consolidation and small airway blockage leading to lung collapse, highlighted by arrows in the upper lobe.
💡 Clinical Takeaways
| Feature | What it indicates |
|---|---|
| Mucoid impaction | Large airway fungal/allergic plugs (e.g., ABPA) or bronchiectasis |
| Tree‑in‑bud | Small-airway infection/inflammation (e.g., TB, PCD, asthma) |
| Atelectasis | Complete blockage, leading to collapse and consolidation |
| Persistent luminal plugs | Associated with worse airflow obstruction and symptoms in COPD/asthma |
✅ Next Steps / Applications
-
These CT examples are valuable for educational use—they illustrate the different patterns seen in mucus plugging across disease types.
-
Radiologists often use these signs to help diagnose and tailor management (infection, allergy, structural lung disease).
-
If your patients or students need simplified visuals, these scans paired with annotations (e.g., arrows, labels) can make great teaching tools.
🧠 What Does It Feel Like?
People often say:
“It felt like something was stuck and wouldn’t come out.”
“I finally coughed up a rubbery strand — like glue.”
“Once it cleared, I could breathe better instantly.”
🧼 How Are Mucus Plugs Treated?
Treatment depends on the underlying cause:
✅ Medications
-
Steroids – reduce inflammation in ABPA and asthma
-
Antifungals – lower fungal load (e.g., itraconazole, posaconazole)
-
Mucolytics – thin mucus (e.g., carbocisteine, hypertonic saline)
-
Antibiotics – treat bacterial infections
✅ Airway Clearance Techniques
-
Respiratory physio – helps you learn how to shift mucus
-
Devices – flutter valve, PEP mask, Acapella
-
Inhaled/nebulised therapy – opens airways and loosens plugs
⚠️ Always speak to your clinical team before starting a new technique.
🧪 Can Coughing Up a Plug Help Diagnosis?
Yes! If you cough up a rubbery, large, or unusual plug, it can be:
-
Tested for fungus, bacteria, or allergy cells (eosinophils)
-
Sent for culture to detect Aspergillus
-
Helpful in guiding or confirming diagnosis of ABPA or Aspergillus bronchitis
👣 Key Points for Aspergillosis Patients
| Question | Answer |
|---|---|
| Is mucus plugging common? | Yes, especially in ABPA, CPA, and bronchiectasis |
| Are all mucus plugs the same? | No – they vary in size, shape, colour, and cause |
| What should I do if I cough one up? | Tell your doctor – it may be useful to test |
| Can it be seen on scans? | Yes – CT can show where plugs are and how severe |
| Can it be treated? | Yes – treatments include steroids, antifungals, mucolytics, and physio |
Other forms of Aspergillosis: 🔬 Acute Invasive Aspergillus Sinusitis (AIAFS)
⚠️ A rare and severe fungal sinus infection — seen almost exclusively in people with severely weakened immune systems
🧾 What is it?
Acute Invasive Aspergillus Sinusitis (AIAFS) is a rapidly progressing fungal infection of the sinuses, caused by Aspergillus species (typically A. fumigatus). It leads to tissue invasion, destruction, and potentially fatal complications if not treated urgently.
🛡️ Who is at Risk of Acute Invasive Aspergillus Sinusitis?
Acute Invasive Aspergillus Sinusitis (AIAFS) is very rare, and affects people who are significantly immunocompromised — meaning their immune systems are unable to control even common environmental fungi.
However, “immunocompromised” is not always black-and-white. There are different degrees of vulnerability, and it's important to understand who is at greatest risk.
🔴 High-risk (severe immunosuppression)
These individuals are at the greatest risk for AIAFS:
-
Profound neutropenia (especially <500 neutrophils/μL for >10 days)
-
Acute leukaemia or stem cell transplantation
-
Solid organ transplant recipients on strong immunosuppressive regimens
-
High-dose corticosteroids (e.g. ≥20 mg prednisolone/day for ≥2 weeks)
-
Uncontrolled HIV/AIDS with low CD4 counts (<200)
-
Diabetic ketoacidosis or severe metabolic acidosis
🟠 Intermediate-risk (chronic or moderate immunosuppression)
Patients in this category may not be at risk of AIAFS, but may still be more vulnerable to chronic or allergic forms of aspergillosis or other infections:
-
Long-term oral corticosteroids at lower doses (e.g. <10 mg/day)
-
Biologic therapies for asthma (e.g. anti-IL-5, anti-IgE), which may subtly modulate immunity
-
Genetic susceptibility (e.g. subtle immune pathway deficiencies identified in CPA or ABPA)
-
COPD, bronchiectasis or severe asthma with impaired local defence
-
Malnutrition or poorly controlled diabetes
These patients are not typically at risk of invasive sinus aspergillosis, but may experience worsening of fungal conditions or atypical presentations of infection.
🟢 Low-risk (normal immune function)
People with normal immune function — even those with:
-
Allergic rhinitis
-
Chronic rhinosinusitis
-
Mild asthma or occasional infections
…are not at risk of developing AIAFS. Everyday exposure to Aspergillus spores is harmless to most people.
💬 Key Clarification:
Having aspergillosis does not automatically mean you are at risk of invasive sinus infection.
Many patients with CPA, ABPA, or SAFS are immunologically “fragile,” but not severely immunocompromised.
AIAFS typically only occurs in people with a combination of immune suppression and a very specific set of risks — especially when white blood cell function is severely impaired.
📋 Symptoms and Signs (typically <4 weeks onset)
-
Fever that does not respond to antibiotics
-
Facial pain or pressure, often severe and one-sided
-
Nasal congestion, discharge (often bloody or blackish)
-
Dark scabs (eschar) on the nasal mucosa or palate
-
Eye swelling, visual changes, or cranial nerve symptoms (if spread to the orbit or brain)
-
Altered mental state, seizures (in advanced cases)
🧪 Diagnosis
AIAFS is diagnosed based on:
-
Clinical suspicion in a high-risk patient
-
Endoscopic examination with biopsy and histology (showing hyphal invasion of tissue)
-
CT/MRI imaging to assess spread (bone, orbit, brain)
-
Culture and molecular testing of sinus material
-
Aspergillus PCR or galactomannan testing may help, but are not definitive alone
💊 Treatment Approach
Treatment must begin urgently, ideally within hours of suspicion.
1. Systemic antifungal therapy
-
First-line: Voriconazole or Isavuconazole
-
Alternatives: Liposomal Amphotericin B
-
Combination therapy may be considered in some cases
-
Therapeutic drug monitoring is essential (especially for voriconazole)
2. Surgical debridement
-
Prompt and aggressive endoscopic surgery is critical
-
Repeat procedures may be needed to remove necrotic tissue
3. Immunological support
-
Reversal of neutropenia if possible (e.g. G-CSF)
-
Reduction or withdrawal of immunosuppressive drugs
-
Management of underlying condition (e.g. glycaemic control in diabetes)
📈 Prognosis
-
Mortality is high (>50%) if not recognised and treated early
-
With rapid antifungal therapy and surgery, survival improves significantly
-
Regular monitoring, follow-up imaging, and immune recovery are crucial to long-term outcomes
🧠 Key Points to Remember
✅ This is a medical emergency, but
✅ It is extremely rare, and
✅ Almost exclusively affects those with profound immune suppression
✅ Not a risk to the general public or people with typical sinus infections
📣 Summary for Patient Awareness
Acute Invasive Aspergillus Sinusitis is very rare.
It is a fast-moving sinus infection caused by a fungus called Aspergillus, but it only happens in people with very weak immune systems, like those having chemotherapy or organ transplants.
It needs urgent treatment with antifungal medicine and sometimes surgery.
If your immune system is normal, this infection is not a risk to you.
Aspergillosis Awareness: Conversation with Tom Bermingham - European Lung Foundation
Conversation with Tom Bermingham - European Lung Foundation
👨 Meet Tom Bermingham
-
Lives in rural County Wexford, Ireland, with his wife.
-
Works as a Rural Development Manager.
-
Diagnosed with aspergillosis in 2022 after years of lung issues.
🌪️ What Triggered His Aspergillosis
-
He grew sunflowers in a polytunnel; handling decaying heads released dust he inhaled.
-
Later, home renovation stirred up bathroom mould/dust—both likely exposures.
🏥 The Path to Diagnosis
-
2019: Hospitalised for cavitating pneumonia and diagnosed with bronchiectasis.
-
Later treated for chronic fatigue syndrome, repeated infections, tiring quickly.
-
Feb 2022: Hospitalised again (17 days), diagnosed with severe adult-onset asthma, oxygen-dependent, with mucus positive for Aspergillus fumigatus.
-
Initially labelled with Chronic Pulmonary Aspergillosis (CPA), treated with steroids, antifungals, inhalers, antibiotics, and fatigue medications.
-
2024: Diagnosis revised to ABPA + Severe Asthma with Fungal Sensitisation (SAFS).
-
October 2024: Hospitalised for COVID-19 and Pseudomonas lung infection treated via PICC line. European Lung Foundation
💔 How It Affects His Daily Life
-
Mornings bring coughing up “dirty mucus” daily—an unsettling reminder.
-
Extreme fatigue, headaches, regular infections dominate his life.
-
Gave up gardening (risk of soil exposure), community work, and physical chores.
-
Lives with constant fear of infection, medication side effects, and hospitalisations.
-
Chronic disease has made long-term planning impossible; relaxation and mental wellbeing are vital.
🧭 How He Manages
-
Supported by his wife and daughters and his flexible employer.
-
Practices listening to his body: rests when needed.
-
Regular check-ups—including CT scans, lung function, sputum and blood tests—keep his care monitored. European Lung Foundation
-
Accepting limitations while focusing on what he can still do helps his mindset.
✅ Key Insights for Aspergillosis Patients
-
Environmental exposures matter: mould, dust, soil may trigger illness—even long after.
-
Diagnosis can be complex and evolve: often overlaps with asthma, bronchiectasis, ABPA, SAFS.
-
Daily life can change significantly, with physical decline and emotional stress.
-
Support network and personalised care are crucial—family, employer flexibility, specialist monitoring.
-
Self-care and mindset: acceptance, rest, and focusing on abilities, not limitations.
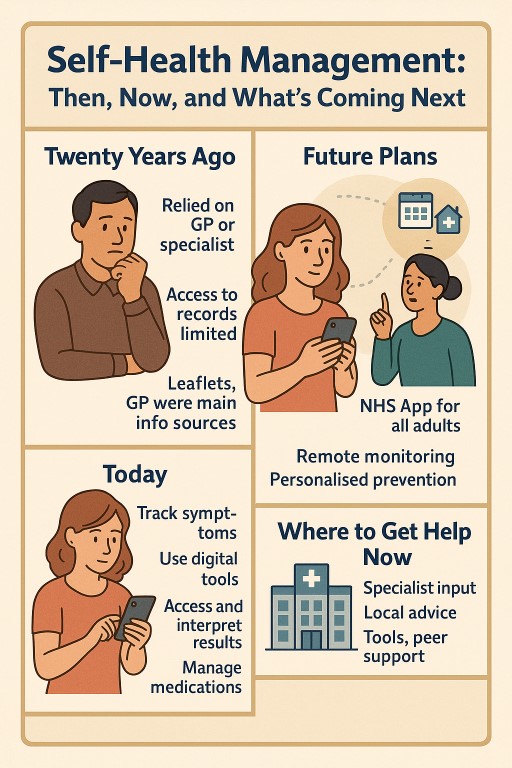
🧭 Self-Health Management: Then, Now, and What’s Coming Next
🧭 Self-Health Management: Then, Now, and What’s Coming Next
Over the past 20 years, the way people manage their health in the UK has changed dramatically — and more changes are on the horizon. For people living with long-term or complex conditions like aspergillosis, asthma, or chronic lung disease, this shift has brought both new opportunities and new burdens.
This article explains what’s changed, what the government is planning, what benefits are hoped for — and what happens if you can’t or don’t want to use online tools.
🕰️ What Was Self-Health Management Like 20 Years Ago?
In the early 2000s:
-
Patients relied heavily on their GP or hospital specialist for every decision.
-
Access to records was limited or non-existent.
-
Health information came from leaflets, GPs, or occasional TV programmes.
-
Appointments were mostly face-to-face and arranged by phone.
-
There was less expectation for people to self-manage complex conditions.
📲 What’s Different Today?
Patients today are expected to:
-
Track symptoms themselves and know when to seek help.
-
Use digital tools like the NHS App, online consultations, and health monitoring apps.
-
Interpret test results, medication side effects, and care plans with less direct support.
-
Coordinate care between services — sometimes across different hospitals or systems.
-
Understand and act on complex health advice, often with less contact from clinicians.
For people with chronic respiratory conditions like CPA or ABPA, this can sometimes improve control — but it can also feel overwhelming, especially when care is fragmented or specialists are hard to reach.
🧑⚕️ How Are Healthcare Staff Adapting?
Many GPs, nurses, and hospital teams are trying to:
-
Embrace shared decision-making and educate patients more directly.
-
Offer video, phone, or online consultations when appropriate.
-
Provide tools like self-monitoring diaries, peak flow meters, or oxygen saturation monitors.
-
Rely on electronic triage systems and limit in-person appointments to the most complex cases.
But many are also under pressure. Staff shortages, long waiting lists, and increased demand mean clinicians have less time per patient, making it harder to offer the detailed guidance many people still need.
🏛️ What Is the UK Government Planning for the Future?
The government’s current plans aim to make the NHS more digital, preventative, and self-directed. This is laid out in the NHS Long Term Plan, the Digital Health and Care Strategy, and the Data Saves Lives policy.
| Goal | Target |
|---|---|
| Make the NHS App the main access point for care | 2025–2026 |
| Move more routine care to remote monitoring and self-management | By 2026–2029 |
| Personalise prevention and reduce avoidable illness | By 2029 |
| Reduce reliance on face-to-face appointments | Ongoing since 2021 |
| Digitise health records across all services | By 2025–2027 |
Patients with long-term conditions are expected to:
-
Manage their own prescriptions
-
Monitor symptoms at home
-
Use digital tools to stay informed and in control
-
Access care only when needed, rather than by default
🎯 What Are the Hoped-For Benefits?
The government promotes these changes as delivering:
✅ Better Outcomes
-
Early intervention, better symptom tracking, and fewer complications.
-
Personalised care plans based on your data and condition.
✅ More Convenient Care
-
Fewer unnecessary visits
-
More control over your own information and appointments
✅ NHS Cost Savings
-
Reducing face-to-face appointments and hospital stays frees up staff time.
-
Less duplication, fewer unnecessary tests, better resource use.
⚠️ But Is It Better for Everyone?
Not necessarily. These benefits are not equally felt by all patients.
🧓 Digital Exclusion Is a Real Problem
-
Around 1 in 5 UK adults struggle with using digital health services.
-
Older adults, people on low incomes, and those with disabilities or learning needs are most affected.
-
Some patients simply don’t feel confident, or don’t trust digital systems.
🧭 What Happens If You’re Left Behind?
Government guidance insists that non-digital options must remain — but this isn’t always consistent. Some patients report:
-
Difficulty reaching practices by phone
-
Online-only booking or consultations
-
Fewer letters and face-to-face reviews
Patients with complex, fluctuating, or rare conditions like aspergillosis may find it harder to get appropriate support without a strong digital presence — especially if care crosses multiple departments or regions.
🧠 So What Needs to Happen?
To make this shift work for everyone, the system must:
-
Protect non-digital access routes (e.g. phone, letter, face-to-face)
-
Offer digital training and support to those who want it
-
Make sure apps and online tools are inclusive and easy to use
-
Involve patients in designing these services — especially those with long-term conditions
-
Keep monitoring for harm or exclusion, and respond quickly
📍 Where Can Patients Get Help Today?
| Support Type | Where to Find It |
|---|---|
| 🔬 Specialist advice | National Aspergillosis Centre, hospital respiratory clinics |
| 👨⚕️ Local support | GP, pharmacist, practice nurse |
| 📱 Digital tools | NHS App, condition-specific apps, NHS websites |
| 🤝 Peer support | Online groups, charities, forums (e.g. Asthma + Lung UK, aspergillosis.org) |
| 💬 Advice lines | NHS 111, condition-specific helplines |
✅ In Summary
The NHS is changing — and patients are expected to change with it. Over 20 years, self-management has gone from optional to expected, and digital care is being rapidly expanded.
For some, this means more control and quicker help. For others, it can feel isolating, confusing, or unsafe. The challenge is to design systems that support everyone — not just the tech-savvy or well-connected.
If you’re living with a long-term condition like aspergillosis, you should never be left managing alone.

🧾 Getting a Second Opinion for Aspergillosis: What If Your Hospital Refuses?
Many patients living with aspergillosis or allergic bronchopulmonary aspergillosis (ABPA) ask for a second opinion — often from a national centre like the National Aspergillosis Centre (NAC) in Manchester or from another specialist elsewhere in the UK. But sometimes, hospitals resist sending your case outside their own department.
Here’s what’s happening, why it might occur, and what you can do.
🤔 Why Would a Hospital Refuse an Outside Opinion?
It’s understandably frustrating when you’ve asked for expert help and your local hospital insists on keeping things “in-house.” Here are some reasons this might happen:
1. Internal Referral Rules
Hospitals sometimes have a policy to refer to another consultant within their own department first. They may consider this a “second opinion,” even if it’s not truly independent.
2. Cost and Complexity
Referrals to another NHS trust — especially across health boards or into England (e.g. to NAC) — can involve extra steps and costs. Some hospitals prefer to avoid that unless they feel there’s no choice.
3. Professional Sensitivities
Some doctors may feel a national second opinion implies criticism of their care, even if your request is made respectfully.
4. Lack of Awareness
Some clinicians aren’t fully aware of what the National Aspergillosis Centre offers — or may underestimate how complex aspergillosis, ABPA, or recurrent fungal infections can be.
🧑⚕️ But Isn’t a Specialist Opinion My Right as an NHS Patient?
Yes. If your GP or hospital team believes it’s clinically appropriate, you have the right to be referred to another NHS consultant — including one outside your local area.
The NAC is nationally commissioned by NHS England to provide care for people with chronic aspergillosis. They accept referrals from across the UK.
💷 Why Private Care Might Not Be an Option
Some patients consider going private when local NHS referrals are blocked — but private care often means:
-
Paying for new scans, blood tests, and sputum cultures
-
No direct access to previous NHS records
-
Higher costs than expected, especially for complex tests
If you can’t afford this, you are not alone, and there are still NHS options available.
🧭 What You Can Do Next
Here are practical steps if you're being blocked from getting a second opinion:
✅ 1. Restate Your Request Clearly
Ask your GP (or write yourself) to reply to the hospital and explain:
-
You are specifically asking for an opinion from a national expert service (e.g. NAC or Dr Iain Page in Edinburgh).
-
This is not a rejection of their care, but a request for specialist reassurance, diagnosis support, or treatment planning.
✅ 2. Ask for a Tertiary Centre Referral
Use the term “tertiary referral” — this means a referral to a national or highly specialised NHS service.
✅ 3. Raise It with PALS
If you're still being blocked, contact your local Patient Advice and Liaison Service (PALS) or NHS complaints team. Explain:
-
You have a rare/complex condition,
-
You’ve asked for a national review,
-
And you’ve been offered only an internal opinion.
✅ 4. Get support on NAC Support Facebook Group
- https://www.facebook.com/groups/aspergillussupport/
💬 In Summary
-
You’re not being difficult — you’re advocating for your health.
-
It is reasonable and often necessary to seek input from specialists like those at the NAC.
-
If you’ve been told “no,” it may be due to policies or misunderstandings — not a reflection on your need for better care.
-
Keep asking, and if needed, involve your GP, or PALS.
Key Shifts to Reinvent the NHS - The 10 Year plan
The plan introduces three radical shifts to modernize the NHS and secure its future:
-
🏥 Hospital → Community
-
Build a Neighbourhood Health Service: community health centres open 6 days/week for 12 hours/day
-
Provide integrated care closer to home—GPs, diagnostics, mental health, rehab, dentists, pharmacists, and even social support
-
Aim to reduce reliance on hospitals and cut waiting lists
-
-
📱 Analogue → Digital
-
Transform the NHS App into a “doctor in your pocket”—for appointments, advice, care plans, and self-referral
-
Embed AI to reduce admin, transcribe consultations, and support clinical decision-making
-
-
🛡️ Sickness → Prevention
-
Emphasize early intervention through more health checks, screenings, vaccines, and public health services
-
Shift funding towards community and preventative care, away from reactive hospital-based services
-
🏗 Underpinning Measures
To support these shifts, the plan introduces:
-
A new operating model & statutory framework to streamline the NHS structure
-
Transparency and accountability through metrics and patient feedback
-
Workforce transformation, including new training and wellbeing support
-
Innovation strategy harnessing genomics, AI, and tech
-
Financial reform via value-based funding—where providers are rewarded for outcomes
🔍 What This Means for You
-
Access to GP advice and care should be faster and more local – with reduced “8 am scramble”
-
More services like scans, mental healthcare, rehab, smoking cessation, and job support delivered at local centres
-
Greater convenience—use the App to manage care, book appointments, or message clinicians
-
Stronger focus on staying healthy—through screening, prevention, and early treatment support
🧩 Challenges & Expert Views
-
Funding & staffing: A £29 billion investment is pledged, but staffing shortages and infrastructure needs remain concerns
-
Implementation: Organisations like the King’s Fund highlight the absence of operational details and worry pilot projects may lead to regional variation
-
Behavioural shift: Success depends on NHS culture evolving—from reactive treatment to proactive, tech-enabled care
✍️ Final Take
The 10‑Year Health Plan represents a transformative vision: bring care closer to home, empower patients digitally, and focus on prevention. With strong backing from Starmer and Health Secretary Streeting, it aims to reshape NHS services by 2035. While optimism is growing, the effectiveness of implementation and securing resources will determine whether it truly delivers for patients and staff.

Taking Charge: How to Get Involved in Decisions About Your Treatment
When you live with a long-term condition like aspergillosis, ABPA, CPA, or severe asthma, you may face tough decisions about medication, side effects, and quality of life. Treatments like biologics can offer huge benefits—but they also carry risks, and no one knows your body, lifestyle, or priorities better than you do.
The NHS is clear in its long-term plan: you should be involved in every major decision about your care. This is known as shared decision-making (SDM), and it means clinicians and patients working together to make the best choices—not just being told what to do.
Here’s how you can become more confident in taking part in your own care—and how to help your clinical team include you.
🪜 Step-by-Step: How to Join the Decision-Making Process
✅ 1. Know You Have a Right to Be Involved
You are not being "difficult" by asking questions or wanting to be part of the decision. The NHS encourages shared decision-making—and it’s your health.
🗣 “I’d like to understand the options and be involved in deciding what’s best for me.”
✅ 2. Ask for the Options – Including None
Sometimes we are only offered one treatment, but most decisions have at least 2 or 3 choices. For example:
-
Start or delay biologics?
-
Try antifungals again or monitor symptoms?
-
Continue with current care or make a change?
Ask:
🗣 “What are my options, including the option of not doing anything right now?”
✅ 3. Talk About What Matters Most to You
Doctors often focus on test results or scan findings. But you may be more concerned about fatigue, side effects, work, travel, or caring for family.
Let them know what your priorities are:
🗣 “My top goal is to stay out of hospital and manage breathlessness so I can keep working.”
🗣 “I can live with minor side effects, but I don’t want something that weakens my immune system too much.”
✅ 4. Understand the Risks and Benefits
Every treatment, including biologics, is a balance—they reduce inflammation but may make you more vulnerable to infection. That doesn’t mean you shouldn’t take them, but it’s important to understand the trade-offs.
Ask:
🗣 “What are the likely benefits of this treatment for someone like me? What are the possible side effects?”
🗣 “How will this affect my overall health and day-to-day life?”
✅ 5. Ask for Time to Reflect
You don’t need to make big decisions in a 10-minute appointment.
🗣 “Can I take this information home and think about it? I’d like to talk with family or other patients before I decide.”
It’s okay to not decide straight away.
✅ 6. Keep Track of Questions and Progress
Write things down before your appointment. You can even bring someone with you, or ask to record the discussion on your phone.
Apps and treatment diaries help you track side effects, symptoms, and goals, so you and your team can review how well things are working later.
✅ 7. Use Supportive Tools and People
Ask for:
-
Leaflets, videos, or trusted websites to read later
-
A follow-up call with a specialist nurse
You could say:
🗣 “Can you recommend a trusted place to read more about this? I’d like to understand it in my own time.”
🧠 A Shift in Thinking: It’s Not About a Quick Fix
We’ve all grown up with advertising that tells us “This treatment will fix the problem.” But in reality, every treatment is a trade-off—between the benefits it brings and the side effects or limitations it may cause.
Even doctors can fall into the trap of focusing only on what they can treat in their specialty—lungs, infections, skin—and miss how treatments affect the whole person.
You can help by:
-
Gently reminding them of the bigger picture
-
Asking them to explain in plain language
-
Saying honestly how things are affecting your life, not just your lungs
🌈 Your Quality of Life Is the Priority
In the end, what matters is how you feel and function. For some, a small side effect might be worth the gain in lung function or fewer flare-ups. For others, it may not. Only you can make that call—with the right information and support.
📌 Good care means making decisions with you, not for you.
📥 Want to Take This Further?
Ask your clinic or GP about:
-
Shared Decision-Making tools (they’re part of NICE guidelines)
-
Getting written summaries of discussions and next steps
And remember: you’re not just a patient—you’re a partner in your care.
Patient Guide: Understanding Aspergillus-Related Chronic Pulmonary Disease
Based on new international guidance (2024)
What is Aspergillus and Why Is It Important?
Aspergillus is a common type of fungus found in the environment. Most people breathe it in every day without any problem. However, if you have a lung condition or a weakened immune system, Aspergillus can cause serious problems. It can:
- Trigger allergic reactions in the lungs
- Infect damaged lung tissue
- Worsen symptoms like coughing, wheezing, or breathlessness
Until recently, doctors treated each type of aspergillus-related lung disease as a separate condition. But new guidance recognises that many patients may have more than one form or sit on a spectrum.
What Conditions Are Included?
The term "aspergillus-related chronic pulmonary disease" covers a range of conditions:
| Condition | What it means |
|---|---|
| ABPA (Allergic Bronchopulmonary Aspergillosis) | An allergic reaction to Aspergillus, usually in asthma or cystic fibrosis patients |
| CPA (Chronic Pulmonary Aspergillosis) | A slow-developing fungal infection, often in people with pre-existing lung damage |
| Aspergillus bronchitis | A fungal infection in the airways, often in people with bronchiectasis |
| Overlap syndromes | Some people show features of more than one of the above |
What Are the Symptoms?
Symptoms can vary, but common signs include:
- Persistent cough (sometimes with mucus or blood)
- Wheezing or breathlessness
- Fatigue and low energy
- Weight loss or loss of appetite
- Repeated chest infections
If you experience these symptoms and have an underlying lung condition, it’s important to ask whether Aspergillus might be involved.
How Is It Diagnosed?
Doctors now use a combination of tests to get a clearer picture:
- Chest CT scan – to look for signs of lung damage or fungal balls
- Sputum samples – to check for the presence of Aspergillus
- Blood tests – to detect allergic antibodies (IgE), immune responses (IgG), or fungal antigens
- Bronchoscopy (sometimes) – to collect samples directly from the lungs
These tests help doctors decide whether it’s an allergic reaction, an infection, or both.
How Is It Treated?
Treatment depends on your symptoms and test results. The aim is to:
- Reduce inflammation
- Clear fungal infection
- Prevent further lung damage
Common treatment options include:
| Treatment | Purpose |
| Steroids (e.g. prednisolone) | Reduce allergic inflammation (especially in ABPA) |
| Antifungal drugs (e.g. itraconazole, voriconazole) | Treat fungal infection and reduce fungal burden |
| Biologic therapies (e.g. omalizumab, dupilumab) | Used in difficult-to-treat allergic cases |
| Nebulised antibiotics | If other infections (like Pseudomonas) are also present |
| Surgery (rarely) | To remove fungal balls or damaged tissue in severe CPA |
What Has Changed in the 2024 Guidance?
- Doctors are now encouraged to look for overlapping features, not just one diagnosis.
- More emphasis is placed on early detection and preventing lung decline.
- Guidelines promote the use of multidisciplinary teams (MDTs) for complex cases.
- Newer treatments, including biologics, are being recommended more often.
- Patients with symptoms but unclear diagnoses should be re-evaluated regularly.
What Can You Do as a Patient?
- Know your diagnosis – Ask your team whether your current label still fits your symptoms
- Track your symptoms – Keep a log of cough, breathlessness, fatigue, and infections
- Ask about specialist referral – For example, to a National Aspergillosis Centre
- Stay informed – Visit aspergillosis.org for up-to-date guidance
- Take medications as prescribed and report any side effects promptly
Support and Information
- Patient support groups can help you connect with others
- Pulmonary rehabilitation and breathing therapy can improve quality of life
- Annual reviews and regular scans can help spot problems early
For more information, leaflets, and help getting the right care, visit: aspergillosis.org
You don’t have to manage this alone.

From Cradle to Shared Care: Understanding the NHS Transition to Patient Partnership
The NHS is evolving. From its early days as a post-war health service built around face-to-face care by a GP who "did it all," to today’s complex model focused on prevention, digital access, and patient partnership — the change has been profound. This document provides a clear overview of why, how, and where the NHS is transitioning toward shared care and self-management.
📜 Then and Now: The 1960s NHS vs Today
The NHS in the 1960s:
- Care was largely reactive — you went to the doctor when you were ill.
- GPs were central and often lifelong figures in a family’s care.
- Most treatments were limited, and few people lived long with chronic illness.
The NHS Today:
- Patients live longer, often with multiple long-term conditions.
- Care must be proactive and coordinated.
- The NHS encourages patients to understand and manage their health.
- The model is increasingly digital, multidisciplinary, and patient-centred.
⚙️ Why the Shift Happened
- Rising Chronic Illness: Diabetes, heart disease, asthma, and mental health issues have all increased.
- Ageing Population: More people need long-term support.
- Advances in Medicine: Enable people to live longer but require more daily self-care.
- Resource Constraints: GP and hospital services are under increasing pressure.
- Better Outcomes with Patient Involvement: Evidence shows shared care leads to better results.
📈 Timeline of Change
| Year | Event |
|---|---|
| 2008–2010 | Expert Patient Programmes piloted |
| 2014 | Five Year Forward View introduces prevention and self-care |
| 2019 | 🚀 NHS Long Term Plan launches personalised care model |
| 2020 | Universal Personalised Care policy published |
| 2021–2022 | COVID accelerates digital triage and remote monitoring |
| 2023–2025 | Integrated Care Systems tasked with delivering shared care |
| 2025 | 📣 Anticipated release of the next major NHS reform report by the current government, expected to include a 10-year plan focusing on community-based care, digital access, and integration with social care |
🧠 What Is Shared Care?
Shared care is a model where:
- Patients are active partners, not passive recipients.
- GPs, nurses, pharmacists, and support workers form a care team.
- People with long-term conditions have personalised care plans.
- Patients are supported to self-monitor and make informed decisions.
📊 Evidence of Impact
- Diabetes & Hypertension: Better control when patients co-manage.
- Asthma & COPD: Action plans reduce flare-ups and hospital visits.
- Mental Health: Shared decision-making improves engagement and outcomes.
- BMJ & Cochrane Reviews: Shared care reduces hospital use and improves satisfaction.
👥 What About Those Without Digital Access?
Digital exclusion affects:
- Older adults
- People with learning difficulties or low literacy
- People without smartphones or broadband
Solutions:
- Maintain paper and telephone options
- Offer face-to-face access when needed
- Train staff to identify and support non-digital patients
- Invest in community digital skills projects
⏳ How Far Along Are We?
We’re mid-transition:
- Policy is in place across England.
- ICSs are developing care coordination teams.
- Self-monitoring and digital records are expanding.
- But delivery is uneven, and many staff need more support and training.
Estimated full embedding of shared care: 2028–2032, depending on region and resources.
🩺 Does the NHS Still Care for Us from Cradle to Grave?
Yes — but with an evolved model:
- Still free at the point of care
- Still lifelong
- But now expects patients to:
- Learn about their condition
- Monitor their health
- Use digital or alternative access routes
- Take shared responsibility for staying well
The shift is from "We’ll do it for you" → to "We’ll support you to do it together."
🏥 The Role of Private Healthcare in the Shared Care Era
Private care plays a growing role alongside the NHS, especially where speed, access, or choice is limited:
Where it helps:
- Faster diagnosis or specialist review
- Choice of clinician and continuity
- Access to treatments not available on the NHS
- Supplementary services like physio or counselling
Limitations:
- Not all can afford it — risk of health inequality
- Poor integration with NHS records
- Standards vary between providers
In context: Private care can complement the NHS, especially for people managing long-term conditions, but it should never replace inclusive, high-quality NHS care. Patients benefit most when systems are coordinated, and no one is left behind.
💷 Will Shared Care Make the NHS and Social Care Cheaper?
In theory, yes — but in practice, it’s more complicated. Shared care and self-management are designed not just to improve health outcomes, but also to reduce long-term demand on overstretched NHS and social care services.
📉 Potential Savings
| Area | How Shared Care Could Save Costs |
| Hospital admissions | Fewer A&E visits and unplanned admissions (e.g. asthma, heart failure) |
| GP appointments | More issues resolved by nurses, pharmacists, or self-care tools |
| Social care needs | Better-managed health can delay or reduce dependency on care packages |
| Medication | Improved adherence and fewer avoidable prescriptions or interactions |
| Workforce efficiency | Tasks redistributed to broader care teams (e.g. care coordinators, link workers) |
⚠️ Upfront Costs to Consider
- Training staff in personalised care and shared decision-making
- Investing in digital systems and patient tools
- Supporting digitally excluded or vulnerable groups
- Funding community-based roles (link workers, social prescribers)
🧮 What the Evidence Says
- The Health Foundation (2021) found that shared care is often cost-effective but savings take years to appear.
- Diabetes Prevention Programmes and home blood pressure monitoring schemes have demonstrated long-term cost reductions when patients are well supported.
- ICSs are beginning to measure value not just in pounds saved, but in avoidable harm and hospital use prevented.
Shared care isn’t a quick fix for NHS finances — it’s an investment in long-term sustainability.
🔗 Do We Need a More Fully Integrated NHS and Social Care?
Yes — integration is essential if shared care is to work effectively.
Currently, NHS healthcare and local authority social care operate through separate budgets, systems, and eligibility rules, which can lead to gaps, delays, or duplication. For patients with complex needs — such as older adults, people with disabilities, or those with long-term conditions — this separation often causes frustration and poorer outcomes.
Why Integration Matters:
- 🧓 Smooth transitions from hospital to home
- 📋 Unified care plans that cover medical, practical, and emotional support
- 🤝 Fewer assessments and handoffs between services
- 💡 Faster responses when needs change
What’s Already Happening:
- Integrated Care Systems (ICSs) aim to bring NHS and social care leaders together
- Some areas are piloting pooled budgets or joint appointments
- Shared care records are being rolled out in regions to link GP, hospital, and social services
Barriers to Integration:
- Separate funding structures (NHS = national, Social Care = local authority)
- Different eligibility rules and charging systems
- Workforce shortages and incompatible IT systems
True shared care requires shared systems, shared responsibility — and shared investment.
🧭 What Support Exists to Help Patients Transition to Shared Care?
As the NHS shifts toward shared care and patient partnership, new support services and resources have been introduced to help patients take on a more active role in their health.
🧑⚕️ Where Patients Can Get Help:
- GP Practices: Many now have a wider team including:
- Care coordinators
- Health and wellbeing coaches
- Social prescribers
- Practice nurses trained in personalised care
- Pharmacies: Community pharmacists can support minor illnesses, medication reviews, and some chronic condition monitoring.
- The NHS App: Allows patients to:
- View medical records
- Order prescriptions
- Access care plans and vaccination status
- Link to symptom checkers and self-care tools
- Patient Support Groups and Charities: Many long-term condition charities (e.g. Asthma + Lung UK, Diabetes UK, Versus Arthritis) offer:
- Peer support
- Online education
- Print resources
- Helplines
- Community Services (varies by area):
- Self-management education courses (e.g. Expert Patients Programme)
- Voluntary sector health coaches or befriending schemes
- Local authority or ICS-run wellbeing hubs
📞 If in Doubt, Ask:
- Contact your GP reception and ask: “Can I speak to someone about managing my condition better?”
- Many areas have health navigators who can connect you to appropriate services.
The transition is not just about expectations — it comes with real support. No one should be left to do it alone.
🎯 Final Thought
The NHS of today — and tomorrow — is built around partnership. While some miss the simplicity of the old model, the future offers tools and support that can help people live longer, healthier lives — if everyone is included. Shared care works best when:
- Patients feel supported
- Clinicians feel equipped
- Services stay flexible and inclusive