by GAtherton
Last reviewed: April 2026…
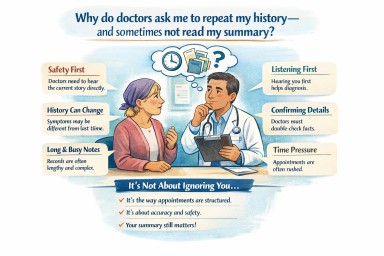
Many people living with…
Last reviewed: 9 April 2026…
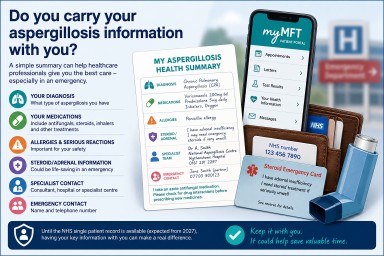
If you live with…
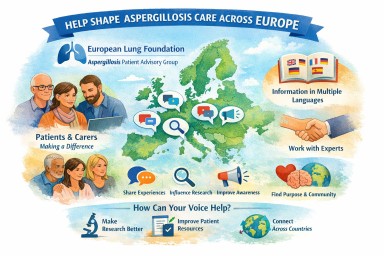
You are not alone with…