Biologics are modern…
by GAtherton
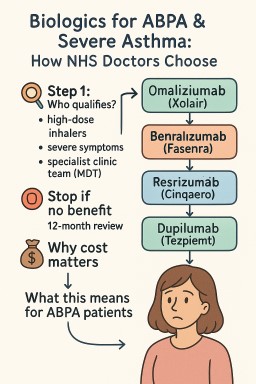
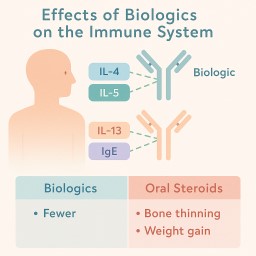
✅ What Are Biologics?…
A guide to when they start…
Many people with ABPA who…
Omalizumab (Xolair) is a…
Biologic medications (also…
[et_pb_section fb_built="1"…