Patient Research

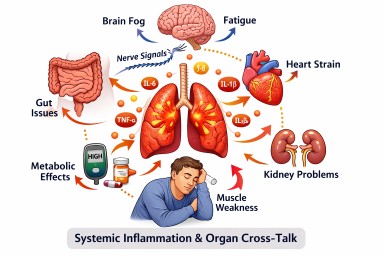
How Inflammation in One Part of the Body Can Affect the Rest of the Body
Last reviewed: 24 March 2026…
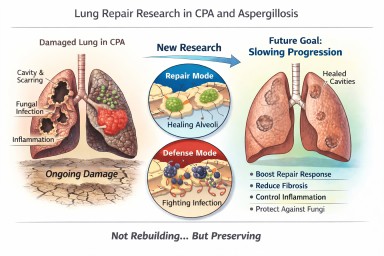
Looking further into the future - could we control lung damage, preserve healthy lung tissue better?
Can Lungs Repair Themselves?…
