Research




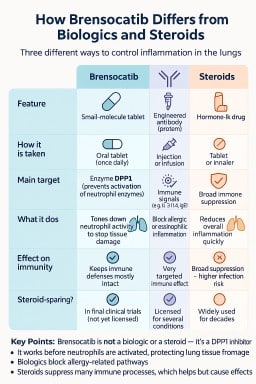
🧬 From Scottish Discovery to American Pharmacy Shelf: The Story of Brensocatib
Sometimes a medicine begins…


🌬️ Inhaled Antifungal Treatments for Chronic Pulmonary Aspergillosis (CPA)
Updated: October 2025 💡 Why…

🧩 NAC Aspergillosis Research Digest Aspergillosis (October 2025: week 43)
Highlights Post‑transplant…

🧩 NAC Aspergillosis Research Digest — Focus: Chronic Aspergillosis (October 2025: week 42)
🧬 Focus Review — Chronic…