Browse information
Latest Articles
Support
For Professionals
Search
Professional Guidance
Home
NAC & Guidance
Archive by Category "Professional Guidance"
Professional Guidance
Weekly Aspergillosis Research Update: New Diagnostics, CAPA Evidence, and Why Azole Tolerance Matters
by GAtherton
About the National Aspergillosis Centre (NAC)
by GAtherton
Why the UK’s Infection Specialist Workforce Matters to People Living with Aspergillosis
by GAtherton
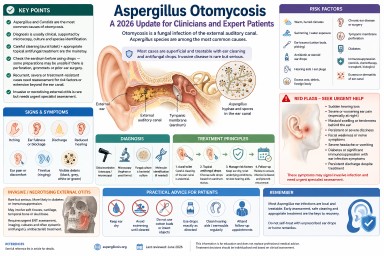
Aspergillus Otomycosis: A 2026 Update for Clinicians and Expert Patients
by GAtherton
More Than a Referral Centre: How the National Aspergillosis Centre Supports Patients and Healthcare Professionals Across the UK
by GAtherton
Professional Aspergillosis Update: May 2026
Audience: respiratory…
by GAtherton
What the UK Infection Workforce Report Means for Aspergillosis Patients and Specialists
by GAtherton
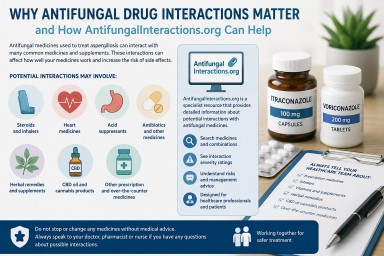
Why Antifungal Drug Interactions Matter — and How AntifungalInteractions.org Can Help
by GAtherton
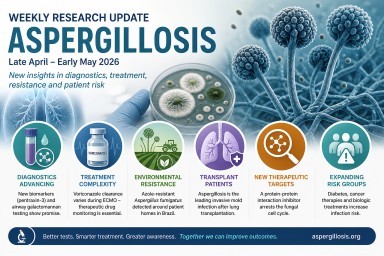
Weekly Aspergillosis Research Update April - May 2026
Search term: aspergillosis…
by GAtherton
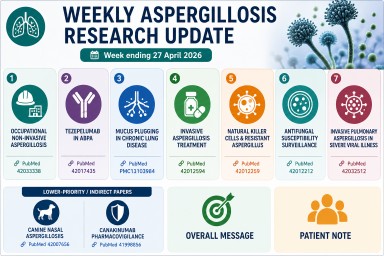
Weekly Aspergillosis Research Update: Week ending 27 April 2026
Highlights this week…
by GAtherton
1
2
3
…
8