Primary immune deficiencies…
by GAtherton
Executive overview (what…
January–February 2026 Search…
World Aspergillosis Day (WAD)…
Grouped by relevance and…
An overview for patients and…
Focusing on what matters most…
How to stay curious,…
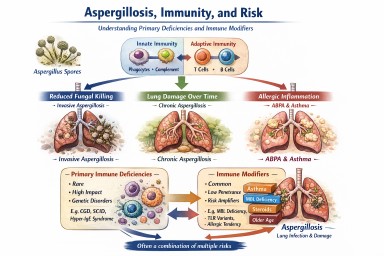
1. Immunodeficiency, rare…
How gut and lung microbiota…