Last reviewed: 18 March 2026…
by GAtherton
Why these infections…
This guide is for people…
A balanced guide for…
A balanced guide for patients…
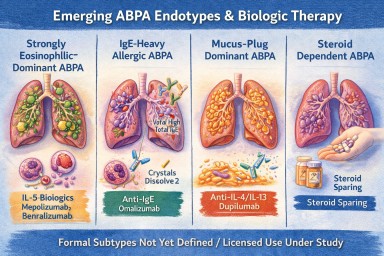
For many years, Allergic…
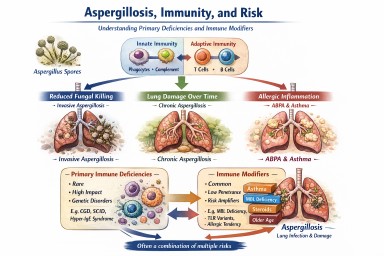
Primary immune deficiencies…