Key points You can have real…
by GAtherton
Last reviewed: April 2026…
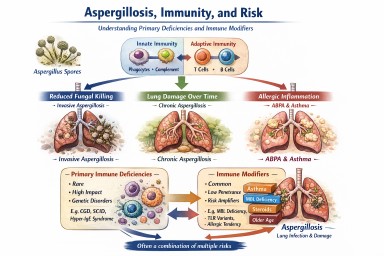
Researchers have recently…
Primary immune deficiencies…
A patient-friendly guide (and…
A Simple Guide for…
A Simple Guide for Patients…
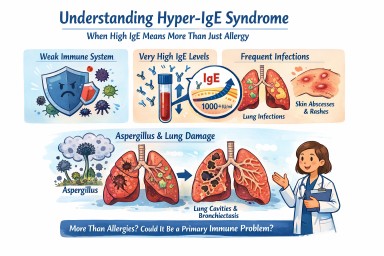
What Aspergillosis Patients…
(Explained with Addison’s…