Browse information
Latest Articles
Support
For Professionals
Search
Other
Home
Conditions
Archive by Category "Other"
Other
NTM and aspergillosis: why are they increasingly found together?
by GAtherton
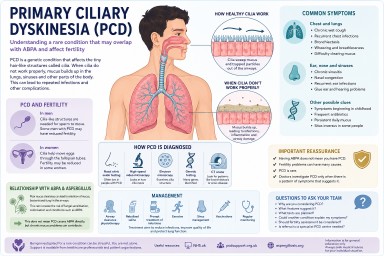
Primary Ciliary Dyskinesia (PCD), Fertility and Aspergillosis
by GAtherton
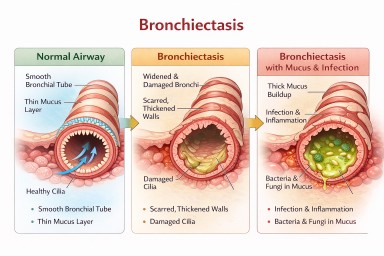
Bronchiectasis in Aspergillosis Patients
Many people with…
by GAtherton