Browse information
Latest Articles
Support
For Professionals
Search
NTM MAC
Home
Posts Tagged "NTM MAC"
NTM MAC
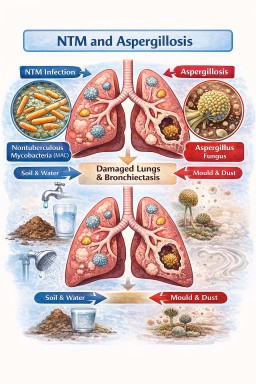
NTM and aspergillosis: why are they increasingly found together?
by GAtherton
Nontuberculous Mycobacteria (NTM–MAC) and Aspergillosis
Why these infections…
by GAtherton