by GAtherton
Last reviewed: 20 March……
This study from the National…
Are they useful yet – and…
A detailed reference for…
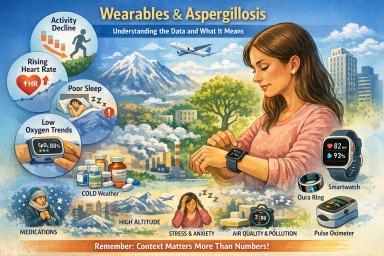
Many people living with…