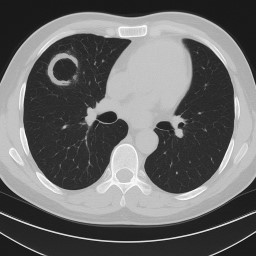
Aspergilloma
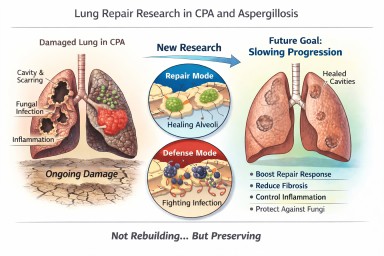
Looking further into the future - could we control lung damage, preserve healthy lung tissue better?
Can Lungs Repair Themselves?…


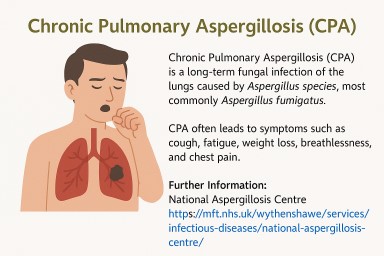
🌬️ Inhaled Antifungal Treatments for Chronic Pulmonary Aspergillosis (CPA)
Updated: October 2025 💡 Why…


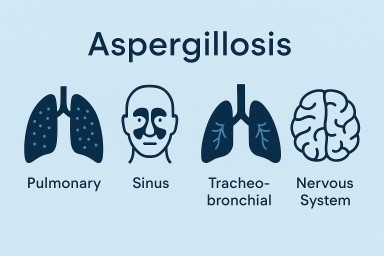
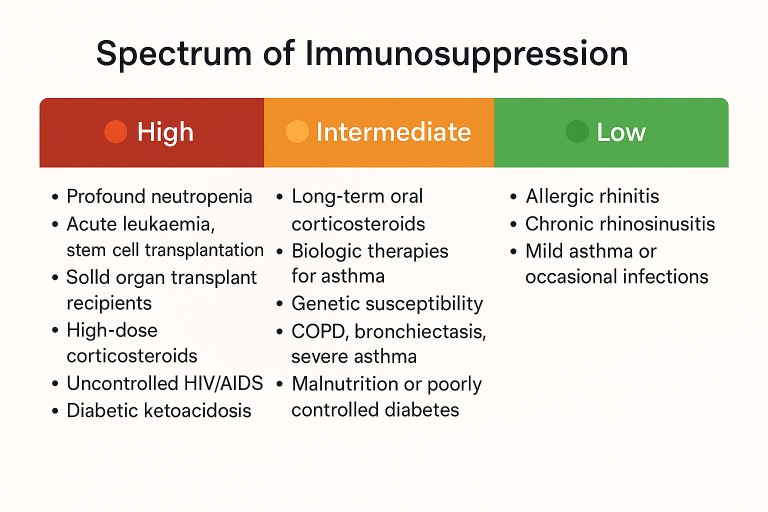
🛡️ Understanding Your Risk: Aspergillosis, Steroids, and the Immune System
If you’ve been diagnosed with…