Browse information
Latest Articles
Support
For Professionals
Search
smoking
Home
Posts Tagged "smoking"
smoking
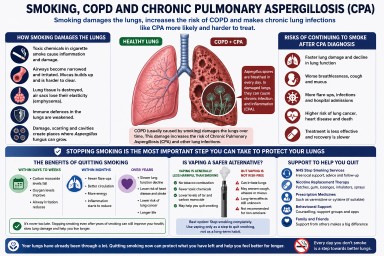
Smoking, COPD and Chronic Pulmonary Aspergillosis (CPA)
by GAtherton