Key points
- Lung function tests show how well your lungs are working, not simply how damaged they look.
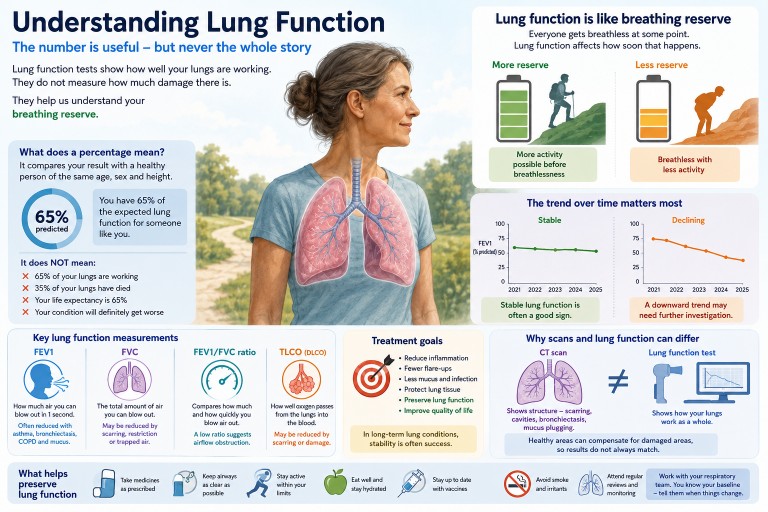
- “60% lung function” usually means 60% of the predicted value for someone of your age, sex and height.
- It does not mean 40% of your lungs have stopped working.
- Everyone loses some lung function naturally with age.
- For many people with aspergillosis or asthma, the trend over time matters more than one single result.
- Successful treatment often means stabilising lung function and preventing further decline.
Contents
- What are lung function tests?
- What does a percentage result mean?
- Lung function as breathing reserve
- Do we naturally lose lung function with age?
- Important lung function results
- What patterns are seen in aspergillosis?
- Why scans and lung function do not always match
- Can treatment stop lung function getting worse?
- When to seek medical help
- Common questions
What are lung function tests?
Lung function tests, also called breathing tests or pulmonary function tests, measure how well your lungs are working.
They can help doctors understand:
- how much air you can breathe out,
- how quickly you can empty your lungs,
- whether your airways are narrowed,
- whether your lungs are restricted or stiff,
- how well oxygen passes from the lungs into the blood.
These tests do not diagnose aspergillosis by themselves. Instead, they are one part of the overall picture, alongside symptoms, CT scans, blood tests, sputum tests, oxygen levels and how active you are day to day.
What does a percentage result mean?
Patients are often told things like:
“Your lung function is 65%.”
This can sound frightening, but it is often misunderstood.
A percentage result usually means your result compared with the value expected for a healthy person of the same:
- age,
- sex,
- height,
- and sometimes ethnic background, depending on the reference system used.
So, if your FEV1 is 65% predicted, it means your measured FEV1 is 65% of the value expected for someone like you.
It does not mean:
- 65% of your lungs are working,
- 35% of your lungs have died,
- you have lost 35% of your life expectancy,
- or that your condition will definitely keep getting worse.
Lung function as breathing reserve
A helpful way to think about lung function is as breathing reserve.
Everyone becomes breathless if they work hard enough. Lung function affects how soon that breathlessness appears.
| Activity | Someone with good breathing reserve | Someone with reduced breathing reserve |
|---|---|---|
| Sitting quietly | Comfortable | Usually comfortable |
| Walking around the house | Comfortable | Usually manageable |
| Shopping | Comfortable or mildly breathless | May need to slow down or pause |
| Climbing stairs | Mildly breathless | More likely to become breathless |
| Walking uphill | Breathless with effort | Breathless sooner and may need rests |
This is why two people with the same lung function percentage can feel very different. Breathlessness is also affected by fitness, weight, muscle strength, heart health, asthma control, mucus, anxiety, anaemia and recent infections.
Do we naturally lose lung function with age?
Yes. Lung function normally peaks in early adulthood and then gradually declines over time.
This happens because of natural changes in:
- lung elasticity,
- the chest wall,
- respiratory muscles,
- and small airways.
However, predicted lung function values already take age into account. This means a 70-year-old is not being compared with a healthy 25-year-old. They are being compared with expected values for someone of similar age, sex and height.
This is why the trend over time is often more useful than a single number.
| Year | FEV1 | Possible interpretation |
|---|---|---|
| 2022 | 64% | Relatively stable |
| 2023 | 63% | |
| 2024 | 65% | |
| 2025 | 62% |
A person may worry about being “only 62%”, while their respiratory team may be reassured that the result has remained stable for several years.
Important lung function results
FEV1
FEV1 stands for Forced Expiratory Volume in One Second.
It measures how much air you can blow out forcefully in the first second after taking a deep breath.
This is often the number people mean when they say, “My lung function is 60%.”
FEV1 is often reduced when airways are narrowed, as in asthma, chronic obstructive pulmonary disease (COPD), bronchiectasis or mucus plugging.
FVC
FVC stands for Forced Vital Capacity.
It measures the total amount of air you can blow out after taking the deepest breath possible.
FVC may be reduced if the lungs cannot expand fully, if there is scarring, restriction, muscle weakness, poor test technique, or if air becomes trapped in the lungs.
FEV1/FVC ratio
The FEV1/FVC ratio compares how much air you blow out in the first second with the total amount you can blow out.
A low ratio usually suggests airflow obstruction. This is common in asthma, COPD and some people with bronchiectasis.
TLCO or DLCO
TLCO or DLCO is often called gas transfer.
It measures how well oxygen passes from the air sacs in the lungs into the bloodstream.
Gas transfer may be reduced by scarring, emphysema, blood vessel problems in the lungs, anaemia, or other lung damage. Sometimes spirometry looks fairly good but gas transfer is reduced, which can help explain breathlessness.
What patterns are seen in aspergillosis?
There is no single “typical” lung function result for aspergillosis patients.
Aspergillosis often develops in people who already have asthma, bronchiectasis, previous tuberculosis, chronic obstructive pulmonary disease, sarcoidosis, prior lung surgery or other lung conditions. This means lung function varies widely from person to person.
Allergic bronchopulmonary aspergillosis (ABPA)
Allergic bronchopulmonary aspergillosis is an allergic inflammatory reaction to Aspergillus, usually in people with asthma or cystic fibrosis.
Lung function may show:
- airflow obstruction,
- reduced FEV1,
- fluctuation during flares,
- improvement after treatment,
- or gradual decline if inflammation and mucus plugging repeatedly damage the airways.
Chronic pulmonary aspergillosis (CPA)
Chronic pulmonary aspergillosis usually occurs in lungs that have already been damaged by another condition.
Lung function may show:
- reduced breathing reserve,
- reduced FVC if there is scarring or volume loss,
- reduced gas transfer,
- or surprisingly preserved spirometry despite abnormal CT scans.
In CPA, stability can be a very positive treatment outcome.
Aspergillus bronchitis
Some people have chronic Aspergillus infection or colonisation in the airways with cough and sputum production.
Symptoms may be troublesome even when lung function changes are modest. This is one reason doctors do not rely on lung function tests alone.
Asthma with Aspergillus sensitisation
Some people with asthma are sensitised to Aspergillus without meeting criteria for ABPA.
Their lung function may vary depending on asthma control, airway inflammation, triggers, inhaler use and recent infections.
Why scans and lung function do not always match
Patients are sometimes told:
“Your CT scan shows quite a lot of damage, but your lung function is better than expected.”
This can happen because CT scans and lung function tests measure different things.
A CT scan shows what the lungs look like. It can show bronchiectasis, scarring, cavities, mucus plugging, nodules or areas of collapse.
Lung function tests show how the lungs work overall.
The lungs have a large reserve capacity. If some areas are damaged but other areas remain healthy, the healthy areas can often compensate. This is why a scan can look alarming while lung function remains better than expected.
The opposite can also happen. A scan may look only mildly abnormal, but the person may feel very breathless because of asthma, small airways disease, poor gas transfer, deconditioning, anaemia, heart disease, anxiety or muscle weakness.
Can treatment stop lung function getting worse?
For many aspergillosis and asthma patients, one of the main aims of treatment is to preserve lung function.
Successful treatment does not always mean lung function returns to normal. It may mean:
- fewer flare-ups,
- less inflammation,
- less mucus plugging,
- fewer infections,
- better symptoms,
- stable CT scans,
- and little or no further decline in lung function.
In allergic bronchopulmonary aspergillosis, treatment aims to reduce inflammation and prevent repeated episodes that can damage the airways.
In chronic pulmonary aspergillosis, antifungal treatment often aims to slow or stop progression, reduce symptoms and preserve remaining lung function.
In asthma, good control with inhalers, biologics where appropriate, trigger reduction and treatment of associated conditions can reduce exacerbations and protect lung health.
For many patients, hearing that lung function is “stable” may sound disappointing. In long-term lung disease, stability is often a very good result.
Small changes are not always meaningful
Lung function tests require effort and technique. Results can vary from day to day.
A small change may reflect:
- how well the test was performed,
- tiredness,
- recent infection,
- asthma control,
- mucus,
- time of day,
- or normal measurement variability.
This is why clinicians look for sustained patterns rather than reacting to every small rise or fall.
Questions to ask your respiratory team
- Which result are we talking about: FEV1, FVC, ratio or gas transfer?
- Is my result stable compared with previous tests?
- Is the pattern obstructive, restrictive, mixed or mainly gas transfer-related?
- Does this result explain my symptoms?
- Could asthma, mucus plugging or infection be affecting today’s result?
- What result would make you concerned about deterioration?
- What can I do to help preserve my lung function?
When to seek medical help
Seek medical advice if you notice:
- a clear and persistent worsening of breathlessness,
- breathlessness at rest or with minimal activity,
- new or worsening wheeze,
- coughing up blood,
- fever or signs of infection,
- new chest pain,
- oxygen levels lower than usual if you monitor them,
- or a sudden drop in exercise tolerance.
Seek urgent medical help if breathlessness is severe, sudden, associated with chest pain, blue lips, confusion, fainting, or oxygen levels are dangerously low compared with your usual readings.
Common questions
What does “60% lung function” mean?
It usually means one of your lung function results is 60% of the value predicted for someone of your age, sex and height. It does not mean only 60% of your lungs are working.
Is there a normal amount of lung function for aspergillosis patients?
No. Aspergillosis patients vary widely. Some have normal or near-normal lung function. Others have severe impairment, often because aspergillosis has developed on top of another lung condition.
Does lower lung function mean I will be more breathless?
Often, yes. Lower lung function usually means less breathing reserve, so you may become breathless with less effort. However, symptoms also depend on fitness, weight, muscle strength, asthma control, mucus, oxygen levels and other health conditions.
Can my lung function improve?
Sometimes. Lung function may improve if asthma control improves, inflammation settles, mucus plugging clears, infection is treated, or fitness improves. Permanent scarring and bronchiectasis are less likely to reverse.
Is stable lung function a good result?
Yes. In long-term lung disease, stable lung function over months or years can be a very positive sign that treatment and monitoring are helping to prevent further deterioration.
Why do I feel worse if my lung function has not changed?
Breathlessness and fatigue can worsen for many reasons, including infection, mucus, asthma flare, anaemia, heart problems, medication side effects, poor sleep, anxiety, pain or loss of fitness. Lung function is important, but it is not the only explanation for symptoms.
Summary
Lung function results are useful, but they need careful interpretation.
The number is not a simple measure of how much lung you have left. It is better understood as a measure of breathing reserve compared with what would be expected for someone like you.
For people with aspergillosis and asthma, the most important question is often not “What is my lung function today?” but “Is my lung function stable over time?”
Many patients live active and fulfilling lives with lung function results that sound worrying when expressed as a percentage. The result matters, but so do symptoms, CT scans, oxygen levels, exercise ability, treatment response and the overall trend.
In long-term lung disease, stability is not failure. Stability can be success.
References and further reading
Author and review information
Written for: aspergillosis.org
Intended audience: People living with aspergillosis, asthma, bronchiectasis or other long-term lung conditions, and their families.
Clinical note: This article is for general education and should not replace advice from your own respiratory team.
Last reviewed: June 2026

Latest News posts
News archive